Treatment Outcome and Prognosis Regarding to MR Pattern and Signal Area in Spinal Cord Injury
- Affiliations
-
- 1Department of Orthopaedic Surgery, College of Medicine, Dong-A University, Busan, Korea. gylee@mail.donga.ac.kr
- KMID: 2040778
- DOI: http://doi.org/10.4184/jkss.2006.13.1.32
Abstract
-
STUDY DESIGN: To determine the capability to predict the clinical manifestations and treatment outcomes of traumatic cervicothoracic cord injury patients based on MR images.
OBJECTIVE
To determine the relationship between the differences in MR patterns and signal areas according to Maravilla and Cohen's classification and the PACS system compared with the Frankel classification, in patients that demonstrated neurologic improvement within 1 year. SUMMARY OF LITERATURE REVIEW: MR is the first imaging modality that directly visualizes the extent of spinal cord derangement, and thus, it has the potential to provide an accurate diagnosis of an injury and to determine the prognosis.
MATERIALS AND METHODS
MR images were evaluated within 3 days of trauma in 36 spinal cord injury patients. The clinical follow-up period was more than 1 year. Quantitative analysis of spinal cord lesions was performed according to the PACS system.
RESULTS
According to Maravilla and Cohen's classification, 36 cases were classified as follows: 8 cases of type I, 10 cases of type II, 9 cases of type III and 9 cases of type IV. There was 1 case of type I, 8 cases of type II, 5 cases of type III, and no cases of type IV, who demonstrated neurologic improvements of more than 1 grade in the Frankel classification. An analysis of the signal areas according to the PACS system demonstrated no cases of areas greater than 100 mm2, 5 cases of areas between 50 to 100 mm2, and 9 cases of areas less than 50 mm2 who demonstrated neurologic improvement.
CONCLUSION
Classification according to the differences between MR imaging and MRI signal areas in patients with spinal cord injuries demonstrated the indicators of neurologic improvement; therefore, we MR imaging can be utilized as a prognostic factor in cases of spinal cord injuries.
Keyword
MeSH Terms
Figure
-

Fig. 1. Quantitative analysis of signal changes on MRI(PACS system). (SD: standard deviation, mean, area : mm2)
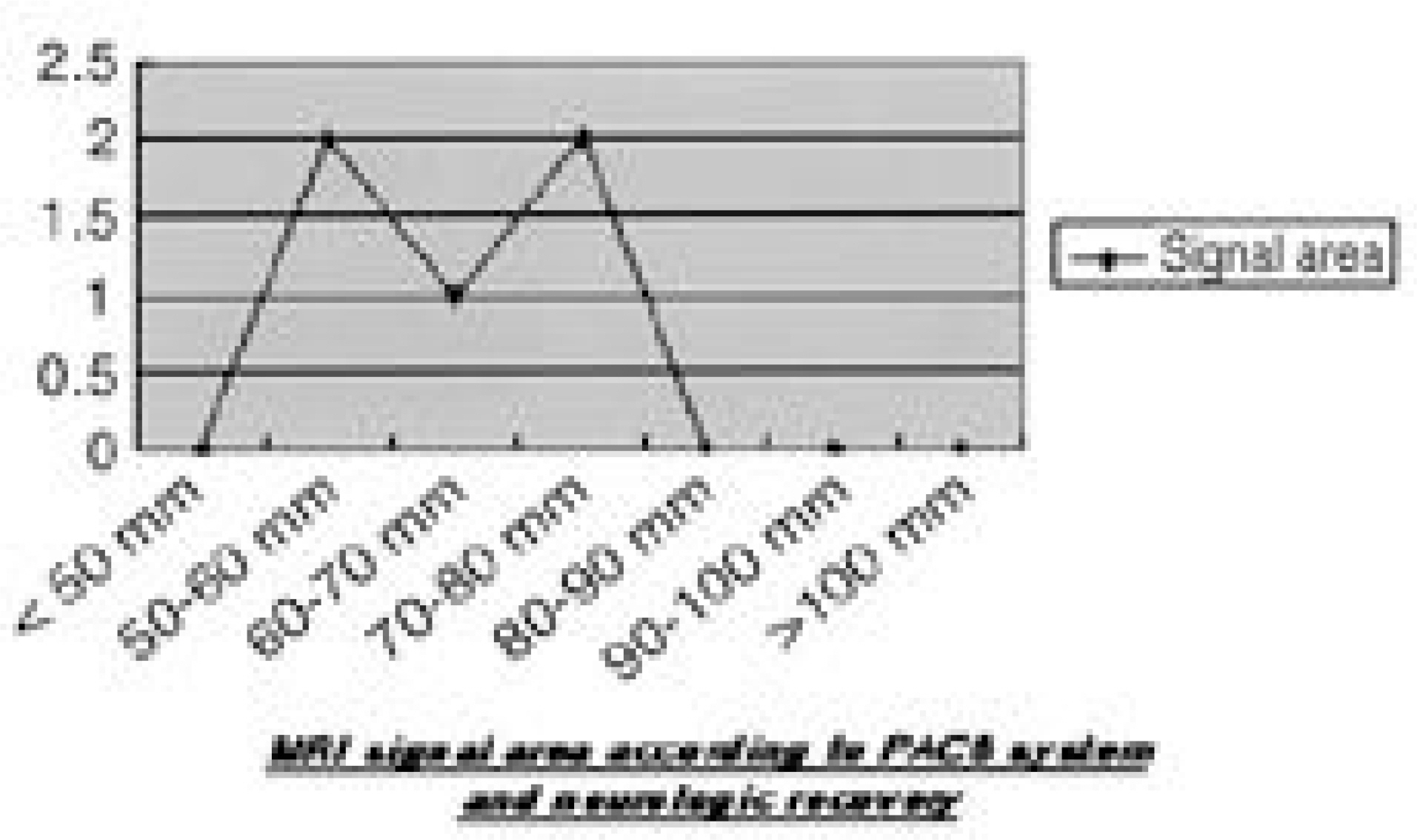
Fig. 2. MR signal area according to PACS system and Neurologic Recovery : Analysis of the signal area according to the PACS system, there were no case of area above 80mm2 who showed neurologic improvement.

Fig. 3. (Type II) MRI of 22-year-old male with C6 tear-drop fracture who become incomplete quadriplegia following incar-TA. Shows neurologic recovery(Frankel grade C to D).(A) T1 isointense (B) Central isosignal, peripheral high (C) Signal range : 62.81mm2

Fig. 4. (Type III) MRI of 50-year-old male with C5-6 fracture and left unilaterl facet joint dislocation who become incomplete quadriplegia following fall down accident. Shows neurologic recovery(Frankel grade B to D).(A) T1: isointense (B) T2: cetral high, peripheral high, C5 level Syringohydromyelia, intramedullary, C4 level (C) Signal range : 40.67mm2

Fig. 5. (Type IV) MRI of 48-year-old male with T11-12 fracture and dislocation who become complete paraplegia following outcar-TA. Not shows neurologic recovery(Frankel grade A to A).(A) T1: transection (B) T2: transection (C) Signal range : >100mm2
Reference
-
1). Blumenkopt B and Juneau PA. Magnetic resonance imaging of thoracolumbar fracture. J Spinal Disorder. 1:144–150. 1988.2). Frankel HL, Hancock DO, Hyslop G, Melzak J, Michaelis LS, Ungar GH, Vernon JD and Walsh JJ. The value of postural reduction in the initial management of closed injuries of the spine with paralplegia and tetraplegia, Part I. Paraplegia. 7:179–192. 1969.3). Melbourne B and Daniel W. Performance analysis of a multicarrier PACS system. Telcordia Technologies 331 Newman Springs Road. Red Bank, NJ 07701, USA.4). Maravilla KR & Cohen WA. MRI Atlas of the spine. London: Martin Dunitz;p. 302–339. 1991.5). Schaefer DM, Flanders AE, Northrup BE, Doan HT and Osterholm JL. Magnetic resonance imaging of acute spinal trauma: Correlation with severity of neurologic injury. Spine. 14:1090–1095. 1988.6). Betz RR, Gelman AJ, DeFilipp GJ, et al. Magnetic reso - nance imaging(MRI) in the evaluation of spinal cord injured children and adolescents. Paraplegia. 25:92–99. 1987.7). Chakeres DW, Flickenger F, Bresnahan JC, et al. MR imaging of acute spinal cord trauma. AJNR. 8:5–10. 1987.8). Dee GJ, Bello JA, Hilal SK. High field, thin section unclear magnetic resonance imaging of the cervical spine. Cardiovasc Intervent Radiol. 8:283–291. 1986.9). Gold berg AL, Rothfus WE, Deeb AL, et al. The impact of magnetic resonance on the diagnostic evaluation of acute cervicothoracic spinal trauma. Skeletal Radiol. 17:89–95. 1988.
Article10). Hackney DB, Asato R, Joseph PM, et al. Hemorrh age and edema in acute spinal cord compression: Demonstration by MR imaging. Radiology. 161:387–390. 1987.11). Mirvis SE. MR provides clues to cervical spine trauma. Diagn Imaging, July. 1988.12). Tarr RW, Drolshagen LF, Kerner TC, et al. MR imaging of recent spinal trauma. Comp Assist Tomogr. 11:412–417. 1987.
Article13). Quencer RM, Sheldon JJ, Post MJD, et al. MRI of the chronically injured cervical spinal cord. AJR. 147:125–132. 1986.
Article14). Vink R, Knoblach SM, Faden AI. 31P magnetic resonance spectroscopy of trumatic spinal cord injury. Magn Reson Med. 5:390–394. 1987.15). Kulkarni MV, McArdle CB, Kopanicky D, Miner M, Cotler H, Lee KF and Harris JH. Acute spinal cord injury: MR imaging at 1.5 T. Radiology. 164:837–843. 1987.
Article16). Osterholm JL. The pathophysiological response to spinal cord injury. J Neurosurg. 40:5–33. 1974.
Article17). Gomori JN, Grossman RI, Goldberg HI, Zimmerman RA and Bilaniuk LT. intracranial hematomas: Imaging by high-field MRI. Radiology. 157:87–93. 1985.18). Koyanagi I, Iwasaki Y, Isu T, Akino M and Abe H. Significance of spinal cord swelling in the prognosis of acute spinal cord injury. Paraplegia. 27:190–197. 1989.19). Shin BJ. Mechanisms and classifications of thoracolumbar fractures. J Korean Spine Surg. 8:392–400. 2001.
Article
