The Modified Chimney Technique With a Thoracic Aortic Stent Graft to Preserve the Blood Flow of the Left Common Carotid Artery for Treating Descending Thoracic Aortic Aneurysm and Dissection
- Affiliations
-
- 1Department of Cardiology, Pusan National University College of Medicine, Busan, Korea. glaraone@hanmail.net
- 2Department of Thoracic and Cardiovascular Surgery, Pusan National University College of Medicine, Busan, Korea.
- 3Department of Anesthesia, Pusan National University College of Medicine, Busan, Korea.
- KMID: 2028768
- DOI: http://doi.org/10.4070/kcj.2012.42.5.360
Abstract
- While thoracic endovascular aortic repair is an effective treatment option for descending thoracic aorta pathology, it does have limitations. The main limitation is related to the anatomical difficulties when disease involves the aortic arch. A fenestrated, branched aortic stent graft and hybrid operation has been introduced to overcome this limitation, but it is a custom-made device and is time consuming to manufacture. Furthermore, these devices cannot be used in an emergency setting. We report two patients with massive descending thoracic aortic aneurysm and ruptured aortic dissection very near the aortic arch who underwent a procedure which we named the modified chimney technique. The modified chimney technique can be used as a treatment option in such an emergency situation or as a rescue procedure when aortic pathology is involved near the supra-aortic vessels.
Keyword
MeSH Terms
Figure
-
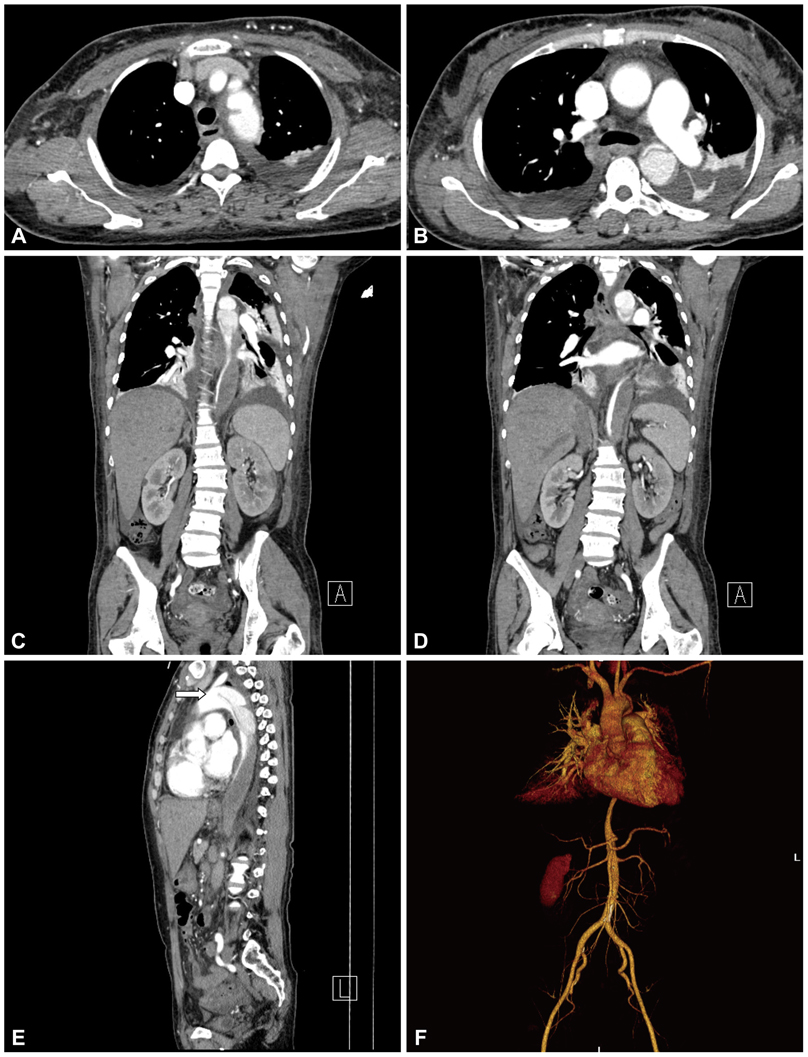
Fig. 1 CT showed a Stanford type B aortic dissection and intramural hematoma at the thoraco-abdominal aorta (A-D). An intimal flap was noted just distal from the left subclavian artery (white arrow in E and F). The intramural hematoma extended to the origin of the renal artery (C).
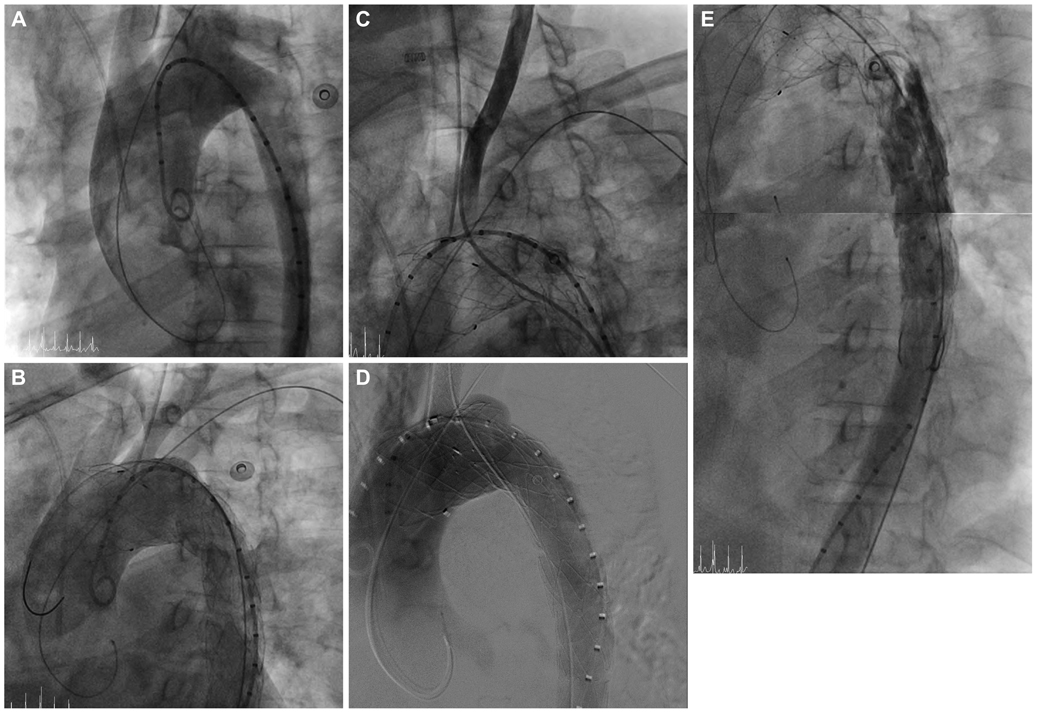
Fig. 2 The overall procedure of the patient. A: the aortogram before stent graft deployment; the proximal entry tear was distal to the LSCA. B: the aortogram after stent graft deployment; the proximal entry tear was completely sealed. The origins of the left carotid artery and LSCA were covered because of the short proximal landing zone. C: selection of the LCCA with a Judkin right 5 Fr catheter through the right femoral artery. D: stent deployment in the LCCA by the chimney graft technique. E: the aortogram after successful stent graft deployment; the occluded true lumen was reexpanded and the false lumen was not seen. The mean pressure gradient between the thoracic and abdominal aorta was decreased to 20 mm Hg from 90 mm Hg after TEVAR. There was no endoleak. TEVAR: thoracic endovascular aortic repair, LSCA: left subclavian artery, LCCA: left common carotid artery.

Fig. 3 The CT scan revealed a Stanford type B aortic dissection combined with a huge aneurysmal dilatation for which the entry site was the aortic arch level and the aneurysm extended to the infrarenal level and ran to the common iliac artery.

Fig. 4 The overall procedure of the patient. A and B: the aortogram before stent graft deployment; the proximal entry tear was distal to the LSCA and there was a huge aneurysm. C: the aortogram after stent graft deployment; the huge aneurysm was completely sealed. The origins of the left carotid artery and LSCA were covered because of the short proximal landing zone. D: selection of the LCCA with a Judkin right 5 Fr catheter through the right femoral artery. E: stent deployment in the LCCA by the chimney graft technique. F: the aortogram after successful stent graft deployment: There was no endoleak. LSCA: left subclavian artery, LCCA: left common carotid artery.
Reference
-
1. Cheng D, Martin J, Shennib H, et al. Endovascular aortic repair versus open surgical repair for descending thoracic aortic disease a systematic review and meta-analysis of comparative studies. J Am Coll Cardiol. 2010. 55:986–1001.2. Malina M, Resch T, Sonesson B. EVAR and complex anatomy: an update on fenestrated and branched stent grafts. Scand J Surg. 2008. 97:195–204.3. Chuter TA, Schneider DB. Endovascular repair of the aortic arch. Perspect Vasc Surg Endovasc Ther. 2007. 19:188–192.4. Sonesson B, Resch T, Allers M, Malina M. Endovascular total aortic arch replacement by in situ stent graft fenestration technique. J Vasc Surg. 2009. 49:1589–1591.5. Criado FJ. Chimney grafts and bare stents: aortic branch preservation revisited. J Endovasc Ther. 2007. 14:823–824.6. Greenberg RK, Clair D, Srivastava S, et al. Should patients with challenging anatomy be offered endovascular aneurysm repair? J Vasc Surg. 2003. 38:990–996.7. Allaqaband S, Jan MF, Bajwa T. "The chimney graft"-a simple technique for endovascular repair of complex juxtarenal abdominal aortic aneurysms in no-option patients. Catheter Cardiovasc Interv. 2010. 75:1111–1115.8. Ohrlander T, Sonesson B, Ivancev K, Resch T, Dias N, Malina M. The chimney graft: a technique for preserving or rescuing aortic branch vessels in stent-graft sealing zones. J Endovasc Ther. 2008. 15:427–432.9. Feezor RJ, Martin TD, Hess PJ, et al. Risk factors for perioperative stroke during thoracic endovascular aortic repairs (TEVAR). J Endovasc Ther. 2007. 14:568–573.10. Rizvi AZ, Murad MH, Fairman RM, Erwin PJ, Montori VM. The effect of left subclavian artery coverage on morbidity and mortality in patients undergoing endovascular thoracic aortic interventions: a systematic review and meta-analysis. J Vasc Surg. 2009. 50:1159–1169.11. Larzon T, Gruber G, Friberg O, Geijer H, Norgren L. Experiences of intentional carotid stenting in endovascular repair of aortic arch aneurysms: two case reports. Eur J Vasc Endovasc Surg. 2005. 30:147–151.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Repair of Thoracic Aortic Aneurysm Using a Custom-made Fenestrated Stent Graft to Preserve the Left Subclavian Artery
- Stent-graft Insertion in High Risk Patients with Aortic Dissection Including Intimal Tear of the Aortic Isthmus: A case report
- Aortic Arch Debranching and Antegrade Stent Graft Placement in an Expanding Distal Dissecting Aneurysm after Repair of an Acute Type I Aortic Dissection
- A Case of Complete Resolution of Aortic Dissection in the Descending Thoracic Aorta Treated with Endovascular Stent-Graft Implantation
- Coarctation of the Aorta Associated with Chronic Thoracic Aortic Aneurysm: A case report
