Reappraisal of intergender differences in the urethral striated sphincter explains why a completely circular arrangement is difficult in females: a histological study using human fetuses
- Affiliations
-
- 1Department of Urology, National Hospital Organization Higashi-Hiroshima Medical Center, Higashi-Hiroshima, Japan. masumoti@hotmail.co.jp
- 2Department of Urology, Tottori University School of Medicine, Yonago, Japan.
- 3Department of Anatomy and Embryology II, Faculty of Medicine, Universidad Complutense, Madrid, Spain.
- 4Division of Internal Medicine, Iwamizawa Kojin-kai Hospital, Iwamizawa, Japan.
- 5Department of Urology, Graduate School of Biomedical Sciences, Hiroshima University, Hiroshima, Japan.
- KMID: 2005869
- DOI: http://doi.org/10.5115/acb.2012.45.2.79
Abstract
- To investigate why the development of a completely circular striated sphincter is so rare, we examined histological sections of 11 female and 11 male mid-term human fetuses. In male fetuses, the striated muscle initially extended in the frontal, rather than in the horizontal plane. However, a knee-like portion was absent in the female fetal urethra because, on the inferior side of the vaginal end, a wide groove for the future vestibule opened inferiorly. Accordingly, it was difficult for the developing striated muscle to surround the groove, even though there was not a great difference in width or thickness between the female vestibule and the male urethra. The development of a completely circular striated sphincter seems to be impossible in females because of interruption of the frontal plane by the groove-like vestibule. However, we cannot rule out the possibility that before descent of the vagina, the urethral striated muscle extends posteriorly.
Figure
-

Fig. 1 Sagittal sections of the fetal urethra and its associated striated muscle (crown-rump lengths, 103 mm). Both (A, female) and (B, male) include a sheet of striated muscle (arrows) restricted to the pubic side of the urethra. The female striated muscle is located at levels superior to the inferior end of the vagina (star in A), while the male muscle attaches to the horizontal urethra proximal to the penile urethra. The female urethra forms a slight curve at the point of merging with the vagina (star in A), while the male urethra clearly changes its direction at the future colliculus as well as on the inferior side of the pubis. A midline fold in the vaginal vestibule (asterisk in A) is the future anterior vaginal column. Hematoxylin and eosin staining. Scale bars=1 mm (A), 5 mm (B).

Fig. 2 Almost horizontal sections of the female urethral striated sphincter. (A) and (B; at the same magnification, scale bar in panel A) display a crown-rump lengths (CRL) 48-mm specimen, while (C) and (D; at the same magnification, scale bar in panel C) show a CRL 100-mm specimen. Panel B (D) is located 0.3 (1.2) mm inferior to panel A (C). Thus, a size difference in the superoinferior axis is evident between these two specimens. The vagina (VAG) merges with the urethra (UR) in (A) and (C). In (B) and (D), the future vaginal vestibule is divided into two lumina by a midline fold, i.e., the anterior vaginal column (star). The urethral striated muscle (rhabdosphincter [RS]) attaches to the lateral aspect of the UR and vestibule. The bulbospongiosus muscle (BS) and the RS are separated by the vestibular bulb (VB in panels B and D). Arrow in (C) or (D) indicates a membranous structure connecting the crus of the clitoris (CR) to the RS. This horizontal plane is slightly tilted (see the double-headed arrow in Fig. 3C). C, clitoris; IC, ischiocavernosus muscle; LA, levator ani muscle; OI, obturator internus muscle; P, pubic bone arch; R, rectum; PN, pelvic nerve plexus. Hematoxylin and eosin staining. Scale bars=1 mm (A, C).
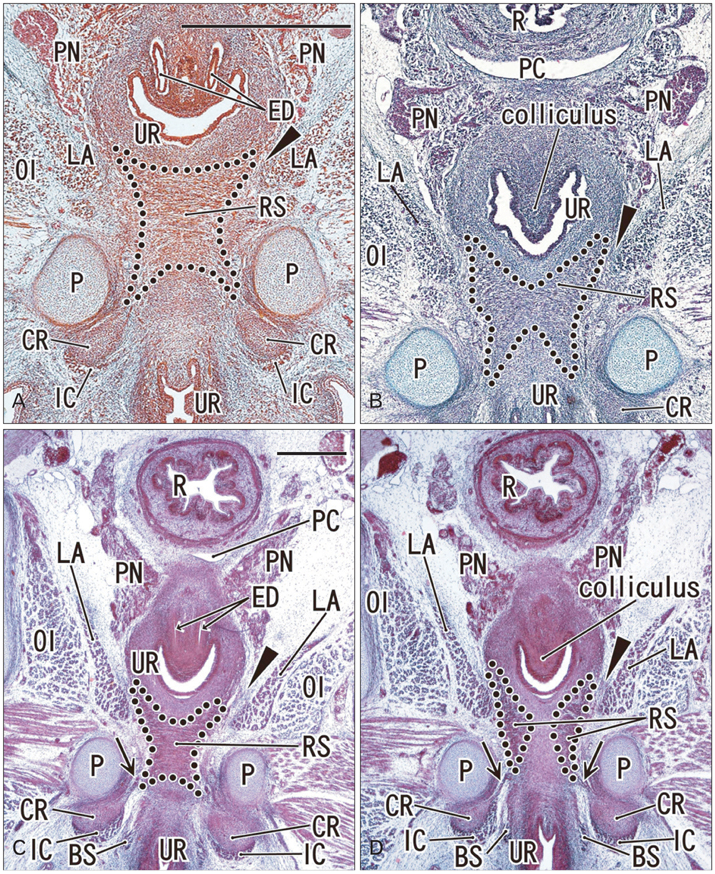
Fig. 3 Almost horizontal sections of the male urethral striated sphincter. Azocarmine (A), azan (B) or hematoxylin and eosin staining (C, D). (A) and (B; at the same magnification, scale bar in panel A) display a crown-rump lengths (CRL) 27-mm specimen, while (C) and (D; at the same magnification, scale bar in panel C) show a CRL 52-mm specimen. Note the distinct difference in size (or scale bar) of these two specimens. Panel B (D), or the inferior aspect of the horizontal urethra, is located 0.1 (0.5) mm inferior to panel A (C), or the superior aspect. The urethral striated muscle (rhabdosphincter [RS]) covers almost all of the horizontal part of the urethra (UR) on the distal side of the colliculus. Both the bulbospongiosus muscle (BS) and the RS are located together along the lateral side of the UR in (D). Arrowheads in all 4 panels indicate loose mesenchymal tissue between the levator ani (LA) and the urethra. Arrows in (C) and (D) indicate a membranous structure connecting between the crus penis (CR) and the RS. This horizontal plane is slightly tilted (see the double-headed arrow in Fig. 3B). ED, ejaculation duct; IC, ischiocavernosus muscle; OI, obturator internus muscle; P, pubic bone arch; PC, peritoneal cavity; PN, pelvic nerve plexus; R, rectum. Scale bars=1 mm (A, C).

Fig. 4 Schematic representations of the fetal urethral striated muscle. (A) The usual concept of the sphincter extending in a horizontal plane. (B) An actual image of the male sphincter extending in the frontal plane but not reaching the inferior aspect of the urethra. This penile urehra directs inferior in contrast to the fetal morphology. (C) The female sphincter overriding the vaginal vestibule. Double-headed arrows in panels (B) and (C) indicate the tilted horizontal planes shown in Figs. 2 and 3. The vestibule is a narrow and deep groove, but here it is drawn concave to emphasize that it opens inferiorly. In all three forms, the urethral striated muscle is located on the inferior or distal side of the point of merging of the genital tract (GT).
Reference
-
1. Strasser H, Ninkovic M, Hess M, Bartsch G, Stenzl A. Anatomic and functional studies of the male and female urethral sphincter. World J Urol. 2000. 18:324–329.2. Kurihara M, Murakami G, Kajiwara M, Taguchi K, Tsukamoto T, Usui T. Lack of the complete circular rhabdosphincter and a distinct circular smooth muscle layer around the proximal urethra in elderly Japanese women: an anatomical study. Int Urogynecol J Pelvic Floor Dysfunct. 2004. 15:85–94.3. Perucchini D, DeLancey JO, Ashton-Miller JA, Galecki A, Schaer GN. Age effects on urethral striated muscle. II. Anatomic location of muscle loss. Am J Obstet Gynecol. 2002. 186:356–360.4. Sebe P, Fritsch H, Oswald J, Schwentner C, Lunacek A, Bartsch G, Radmayr C. Fetal development of the female external urinary sphincter complex: an anatomical and histological study. J Urol. 2005. 173:1738–1742.5. Masumoto H, Rodríguez-Vázquez JF, Verdugo-López S, Murakami G, Matsubara A. Fetal topographical anatomy of the female urethra and descending vagina: a histological study of the early human fetal urethra. Ann Anat. 2011. 193:500–508.6. Oelrich TM. The striated urogenital sphincter muscle in the female. Anat Rec. 1983. 205:223–232.7. Kato M, Matsubara A, Murakami G, Abe S, Ide Y, Sato I, Usui T. Female perineal membrane: a study using pelvic floor semiserial sections from elderly nulliparous and multiparous women. Int Urogynecol J Pelvic Floor Dysfunct. 2008. 19:1663–1670.8. Kato M, Niikura H, Yaegashi N, Murakami G, Tatsumi H, Matsubara A. Histotopography of the female cavernous nerve: a study using donated fetuses and adult cadavers. Int Urogynecol J Pelvic Floor Dysfunct. 2008. 19:1687–1695.9. O'Rahilly R, Müller F. Human embryology and teratology. 1996. 2nd ed. New York: Wiley-Liss.10. Hirata E, Fujiwara H, Hayashi S, Ohtsuka A, Abe S, Murakami G, Kudo Y. Intergender differences in histological architecture of the fascia pelvis parietalis: a cadaveric study. Clin Anat. 2011. 24:469–477.11. Hirata E, Koyama M, Murakami G, Ohtsuka A, Abe S, Ide Y, Fujiwara H, Kudo Y. Comparative histological study of levels 1-3 supportive tissues using pelvic floor semiserial sections from elderly nulliparous and multiparous women. J Obstet Gynaecol Res. 2011. 37:13–23.12. Valasek P, Evans DJ, Maina F, Grim M, Patel K. A dual fate of the hindlimb muscle mass: cloacal/perineal musculature develops from leg muscle cells. Development. 2005. 132:447–458.13. Sasaki C, Yamaguchi K, Akita K. Spatiotemporal distribution of apoptosis during normal cloacal development in mice. Anat Rec A Discov Mol Cell Evol Biol. 2004. 279:761–767.14. Yamaguchi K, Kiyokawa J, Akita K. Developmental processes and ectodermal contribution to the anal canal in mice. Ann Anat. 2008. 190:119–128.15. Arakawa T, Murakami G, Nakajima F, Matsubara A, Ohtsuka A, Goto T, Teramoto T. Morphologies of the interfaces between the levator ani muscle and pelvic viscera, with special reference to muscle insertion into the anorectum in elderly Japanese. Anat Sci Int. 2004. 79:72–81.16. Nakajima F, Takenaka A, Uchiyama E, Hata F, Suzuki D, Murakami G. Macroscopic and histotopographic study of the deep transverse perineal muscle (musculus transversus perinei profundus) in elderly Japanese. Ann Anat. 2007. 189:65–74.17. Oelrich TM. The urethral sphincter muscle in the male. Am J Anat. 1980. 158:229–246.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anatomical Features of Male Rat Urethra and Comparison of Urethral Sphincter Contractility according to Different Urethral Strip Orientations
- Clinical and Functional Anatomy of the Urethral Sphincter
- Effect of Transrectal Probe Insertion on the Opening of Internal Urethral Sphincter
- Dynamic Urethral Pressure Profilometry using Triple Lumen Urodynamic Catheter
- Ultrastructural Study on Transitional Zone of Esophageal Skeleto-Smooth Muscle in Rodents
