Clinical Usefulness of Doppler Ultrasonography before Percutaneous Transluminal Angioplasty for Immature Native Arteriovenous Fistula
- Affiliations
-
- 1Department of Radiology, Inje University Seoul Paik Hospital, College of Medicine, Inje University, Seoul, Korea.
- 2Department of Radiology, Eulji General Hospital, College of Medicine, Eulji University, Seoul, Korea. ykchoman@eulji.ac.kr
- 3Department of Nephrology, Eulji General Hospital, College of Medicine, Eulji University, Seoul, Korea.
- KMID: 2002855
- DOI: http://doi.org/10.3348/jksr.2013.69.5.351
Abstract
- PURPOSE
To report the clinical efficacy of preprocedural doppler ultrasound examination for the treatment of immature arteriovenous fistula by means of percutaneous transluminal angioplasty (PTA) and the efficacy of PTA about its treatment.
MATERIALS AND METHODS
From November 2008 to May 2013, 28 patients who were diagnosed with immature arteriovenous fistula using doppler ultrasound examination and obtained successful maturation of it after PTA were included in this study. A retrospective comparative analysis was performed according to the findings between doppler ultrasound examination and fistulography during the procedure. The success rate of PTA and patency of fistula were evaluated in each patient.
RESULTS
Doppler ultrasound examination revealed stenosis in twenty three patients and thrombotic total occlusion in five patients. Stenosis was located in the proximal cephalic vein 2 cm from the anastomosis in 67.8% (19/28). In the five cases of thrombotic total occlusion, the lesions were long lesions from the anastomosis to the entire proximal cephalic vein at the elbow joint level. Fistulography revealed 5 patients with thrombotic total occlusion and 24 stenosis sites in 23 patients, respectively. The location and characteristics of all lesions were consistent on doppler ultrasound examination. Only four cases were observed as non-thrombotic total occlusion on fistulography, which had more than 90% stenosis on doppler ultrasound examination. The initial success rate of PTA for immature arteriovenous fistula was 96.4% (27/28). In three patients, clinical success was obtained after four times of additional PTA. Six additional PTAs were performed during follow-up, no complications related to the procedures were found. The primary patency rate was 92.9% at 3 months, 60.7% at 6 months and 39.3% at 12 months. The estimated mean survival of arteriovenous fistula was 347.9 days and the estimated median survival was 232 days. Also, the 12 months primary patency rates between the stenosis group and occlusion group showed no significant statistical difference.
CONCLUSION
Assessment of immature arteriovenous fistula using doppler ultrasound examination is a very useful method that can replace diagnostic fistulography. Also, PTA of immature arteriovenous fistula is considered an effective initial treatment for inducing successful growth maturation.
MeSH Terms
Figure
-

Fig. 1 An 80-year-old male with immature radiocephalic arteriovenous fistula. A. The gray-scale of doppler ultrasonography shows a diameter of anastomosis, a serial caliber difference of proximal venous limb and depth of fistula. B. The pulse wave doppler measurement shows a small volume flow along proximal venous limb of fistula.

Fig. 2 A 51-year-old male with immature radiocephalic arteriovenous fistula (AVF). Comparison between color doppler ultrasound examination and angiography. A. The color doppler ultrasonography shows a less 2 mm diameter of anastomosis and proximal venous limb of radiocephalic AVF (arrowheads). B. The angiography after puncture of left brachial artery shows a focal severe stenosis of proximal venous limb of radiocephalic AVF (arrows).
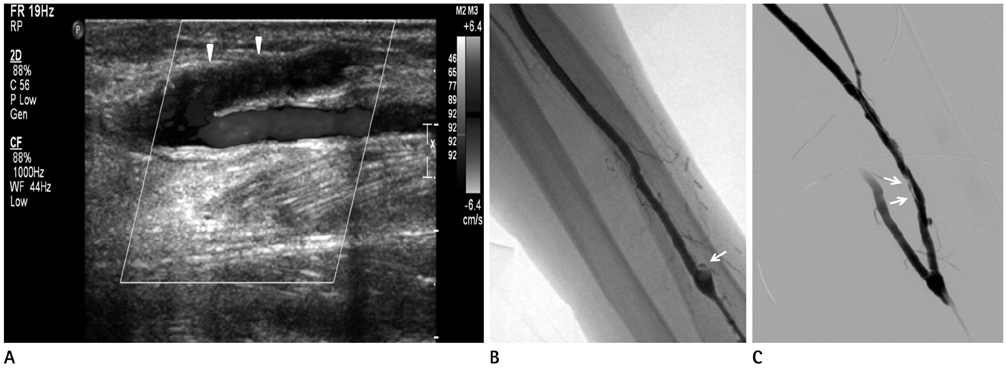
Fig. 3 A 77-year-old male with immature radiocephalic arteriovenous fistula (AVF). Comparison between color doppler ultrasound examination and angiography of totally thrombotic occluded radiocephalic AVF. A. The color-scale longitudinal doppler ultrasonography shows a totally occluded flow and large amount of echogenic thrombus through entire proximal venous limb of fistula (arrowheads). B. The angiography after puncture of left brachial artery shows a totally occluded proximal venous limb of fistula from just distal from anastomosis (arrow). C. After percutaneous balloon angioplasty with 3 mm × 15 cm balloon catheter, the final angiography shows a completely recanalized entire proximal venous limb of fistula without residual stenosis, but small amount remained thrombi was observed around venous wall of proximal venous limb of fistula (arrows).

Fig. 4 A 78-year-old male with a pseudoaneurysm of proximal venous limb of radiocephalic arteriovenous fistula (AVF) after percutaneous transluminal angioplasty (PTA). A. The angiography after puncture of brachial artery shows a focal severe stenosis of proximal venous limb of immature radiocephalic AVF (arrowhead). B. After PTA with 3.0 mm × 4 cm balloon catheter, the final angiography shows an acute onset of pseudoaneurysm at most stenosis site of proximal venous limb of immature radiocephalic AVF (arrow).
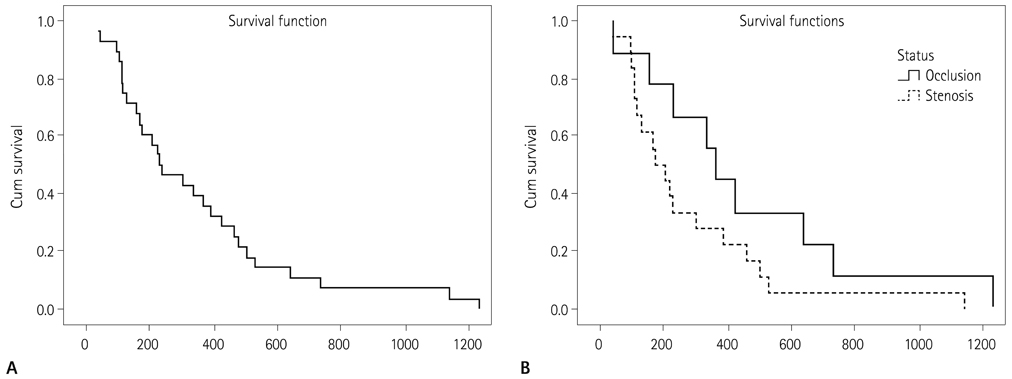
Fig. 5 Clinical success analysis of all patients. A. Kaplan-Meier estimation of primary patency of arteriovenous fistula after percutaneous transluminal angioplasty. B. The Log Rank test estimation of statistical difference between stenosis group and occlusion group.
Reference
-
1. Vascular Access 2006 Work Group. Clinical practice guidelines for vascular access. Am J Kidney Dis. 2006; 48:Suppl 1. S176–S247.2. Asif A, Roy-Chaudhury P, Beathard GA. Early arteriovenous fistula failure: a logical proposal for when and how to intervene. Clin J Am Soc Nephrol. 2006; 1:332–339.3. Nassar GM. Endovascular management of the "failing to mature" arteriovenous fistula. Tech Vasc Interv Radiol. 2008; 11:175–180.4. Beathard GA. An algorithm for the physical examination of early fistula failure. Semin Dial. 2005; 18:331–335.5. Beathard GA, Arnold P, Jackson J, Litchfield T. Physician Operators Forum of RMS Lifeline. Aggressive treatment of early fistula failure. Kidney Int. 2003; 64:1487–1494.6. Gadallah MF, Paulson WD, Vickers B, Work J. Accuracy of Doppler ultrasound in diagnosing anatomic stenosis of hemodialysis arteriovenous access as compared with fistulography. Am J Kidney Dis. 1998; 32:273–277.7. Robbin ML, Chamberlain NE, Lockhart ME, Gallichio MH, Young CJ, Deierhoi MH, et al. Hemodialysis arteriovenous fistula maturity: US evaluation. Radiology. 2002; 225:59–64.8. Singh P, Robbin ML, Lockhart ME, Allon M. Clinically immature arteriovenous hemodialysis fistulas: effect of US on salvage. Radiology. 2008; 246:299–305.9. Turmel-Rodrigues L, Mouton A, Birmelé B, Billaux L, Ammar N, Grézard O, et al. Salvage of immature forearm fistulas for haemodialysis by interventional radiology. Nephrol Dial Transplant. 2001; 16:2365–2371.10. Kim YO, Song HH, Kim NI, Yoon SA, Song HC, Choi EJ, et al. The effect of percutaneous angioplasty on the treatment of poor maturation of the native arteriovenous fistula. Korean J Med. 2000; 59:40–46.11. Chung JY, Song HH, Kim KT, Kim YO, Yoon SA. Efficacy of percutaneous transluminal angioplasty for treating non-maturing brescia-cimino fistulas. J Korean Radiol Soc. 2004; 51:281–290.12. Miller GA, Hwang W, Preddie D, Khariton A, Savransky Y. Percutaneous salvage of thrombosed immature arteriovenous fistulas. Semin Dial. 2011; 24:107–114.13. Lockhart ME, Robbin ML. Hemodialysis access ultrasound. Ultrasound Q. 2001; 17:157–167.14. Gray RJ, Sacks D, Martin LG, Trerotola SO. Society of Interventional Radiology Technology Assessment Committee. Reporting standards for percutaneous interventions in dialysis access. J Vasc Interv Radiol. 2003; 14(9 Pt 2):S433–S442.15. Aruny JE, Lewis CA, Cardella JF, Cole PE, Davis A, Drooz AT, et al. Quality improvement guidelines for percutaneous management of the thrombosed or dysfunctional dialysis access. J Vasc Interv Radiol. 2003; 14(9 Pt 2):S247–S253.16. Manninen HI, Kaukanen E, Mäkinen K, Karhapää P. Endovascular salvage of nonmaturing autogenous hemodialysis fistulas: comparison with endovascular therapy of failing mature fistulas. J Vasc Interv Radiol. 2008; 19:870–876.17. Mercado C, Salman L, Krishnamurthy G, Choi K, Artikov S, Thomas I, et al. Early and late fistula failure. Clin Nephrol. 2008; 69:77–83.18. Falk A, Teodorescu V, Lou WY, Uribarri J, Vassalotti JA. Treatment of "swing point stenoses" in hemodialysis arteriovenous fistulae. Clin Nephrol. 2003; 60:35–41.19. Alamdaran A, Nazemian F, Taheri H. Doppler ultrasound assessment of well-functioning native hemodialysis access: comparison with sufficient dialysis. Iran J Radiol. 2008; 5:101–105.20. Pietura R, Janczarek M, Zaluska W, Szymanska A, Janicka L, Skublewska-Bednarek A, et al. Colour Doppler ultrasound assessment of well-functioning mature arteriovenous fistulas for haemodialysis access. Eur J Radiol. 2005; 55:113–119.21. Ascher E, Hingorani A, Marks N. Duplex scanning-derived access volume flow: novel predictor of success following endovascular repair of failing or nonmaturing arteriovenous fistulae for hemodialysis. Vascular. 2010; 18:9–13.22. Ives CL, Akoh JA, George J, Vaughan-Huxley E, Lawson H. Pre-operative vessel mapping and early post-operative surveillance duplex scanning of arteriovenous fistulae. J Vasc Access. 2009; 10:37–42.23. Bay WH, Henry ML, Lazarus JM, Lew NL, Ling J, Lowrie EG. Predicting hemodialysis access failure with color flow Doppler ultrasound. Am J Nephrol. 1998; 18:296–304.24. Wiese P, Nonnast-Daniel B. Colour Doppler ultrasound in dialysis access. Nephrol Dial Transplant. 2004; 19:1956–1963.25. Middleton WD, Picus DD, Marx MV, Melson GL. Color Doppler sonography of hemodialysis vascular access: comparison with angiography. AJR Am J Roentgenol. 1989; 152:633–639.26. Lumsden AB, MacDonald MJ, Kikeri D, Cotsonis GA, Harker LA, Martin LG. Prophylactic balloon angioplasty fails to prolong the patency of expanded polytetrafluoroethylene arteriovenous grafts: results of a prospective randomized study. J Vasc Surg. 1997; 26:382–390. discussion 390-392.27. Yerdel MA, Kesenci M, Yazicioglu KM, Döşeyen Z, Türk-çapar AG, Anadol E. Effect of haemodynamic variables on surgically created arteriovenous fistula flow. Nephrol Dial Transplant. 1997; 12:1684–1688.28. Kian K, Vassalotti JA. The new arteriovenous fistula: the need for earlier evaluation and intervention. Semin Dial. 2005; 18:3–7.29. Hong HP, Kim SK. Usefulness of percutaneous intervention with transarterial approach in the salvage of nonmaturing native fistulas status-post transvenous approach failure: transarterial approach in the salvage of nonmaturing native fistulas. Cardiovasc Intervent Radiol. 2009; 32:1252–1256.30. Liang HL, Pan HB, Chung HM, Ger LP, Fang HC, Wu TH, et al. Restoration of thrombosed Brescia-Cimino dialysis fistulas by using percutaneous transluminal angioplasty. Radiology. 2002; 223:339–344.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of an Immature Autogenous Arteriovenous Fistula with Percutaneous Transluminal Angioplasty
- A case of arteriovenous fistula with drainage into the coronary sinus during the percutaneous tranluminal coronary angioplasty of chronic total occlusion of circumflex coronary artery
- Erratum: Clinical Usefulness of Doppler Ultrasonography before Percutaneous Transluminal Angioplasty for Immature Native Arteriovenous Fistula
- An Iatrogenic Coronary Arteriovenous Fistula Caused by Guidewire Trauma during Percutaneous Coronary Intervention
- On Postoperative Day Balloon Angioplasty for Salvage of Newly-Placed, Flow-Limiting Native Arteriovenous Fistula
