Korean J Urol.
2007 Apr;48(4):422-427. 10.4111/kju.2007.48.4.422.
Relationship between the Success of Extracorporeal Shock Wave Lithotripsy (ESWL) and the Degree of Hydronephrosis when Treating Patients with Upper Ureteral Stones
- Affiliations
-
- 1Department of Urology, College of Medicine, Chosun University, Gwangju, Korea. mu-hn@daum.net
- KMID: 1997110
- DOI: http://doi.org/10.4111/kju.2007.48.4.422
Abstract
- PURPOSE
We tried to determine the relation between the degree ofstone- induced hydronephrosis and the outcome of extracorporeal shock wave lithotripsy (ESWL) when treating patients with solitary upper ureteral stone.
MATERIALS AND METHODS
260 proximal ureteral stone patients with or without hydronephrosis were treated with ESWL between January 2003 and December 2006 and 8 of these patients were lost to follow up. The degree of hydronephrosis was defined by performing renal ultrasound. The patients were divided into four groups according to the degree of hydronephrosis. Group 0 (n=30) had no urinary system dilatation, group 1 (n=123) had a mild dilatation of the renal pelvis but no renal calices, group 2 (n=75) had a moderate dilatation of the renal pelvis and group 3 (n=24) had a severe dilatation of the renal pelvis and calices. In addition to the degree of hydronephrosis, the stone size, number of sessions, number of shockwave treatments applied and the success rate of ESWL were recorded.
RESULTS
The success rate after ESWL treatment was 92.9% (n=234). There were no statistically significant differences among the groups for the stone size, number of sessions and number of applied shockwave treatments. There were a trend for a decreased success rate of ESWL with an increased degree of hydronephrosis, but this did not reach statistical significance (p=0.436). After ESWL, a few patients encountered minor complications such as gross hematuria, flank pain, stone street, fever and perirenal hematoma. Yet most cases were treated conservatively and there was no need for hospitalization.
CONCLUSIONS
For the patients in our study who had a solitary calculus in the upper ureter, the degree of hydronephrosis caused by the stone does not affect the success rate after ESWL.
MeSH Terms
Figure
-
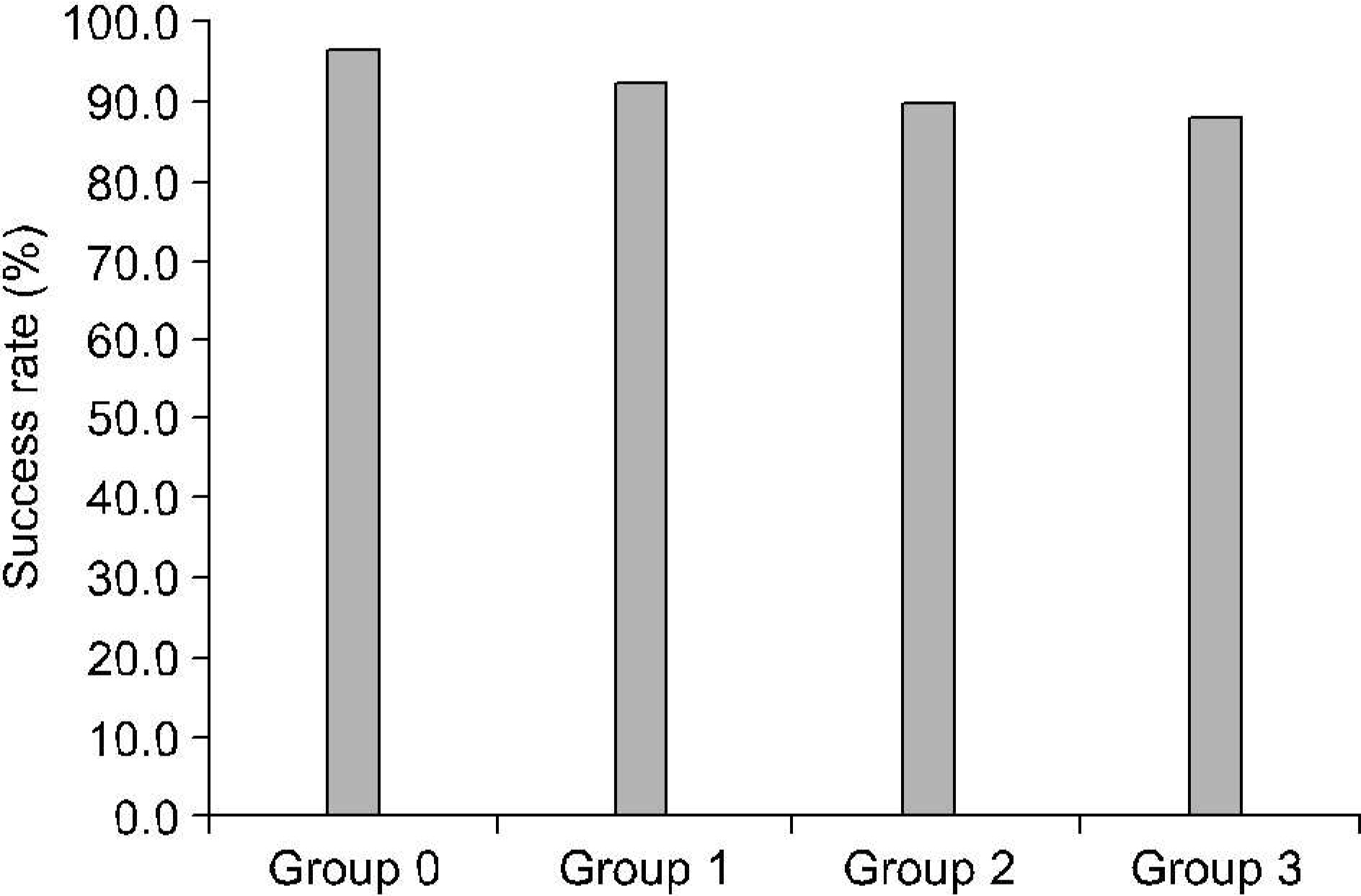
Fig. 1. Success rate of extracorporeal shock wave lithotripsy (ESWL) between the four groups (p=0.436). Group 0 had no urinary system dilatation, group 1 had a mild dilatation of the renal pelvis but not renal calices, group 2 had a moderate dilation of the renal pelvis and group 3 had a severe dilatation of the renal pelvis and calices.
Reference
-
1.Chaussy C., Brendel W., Schmiedt E. Extracorporeally induced destruction of kidney stones by shock waves. Lancet. 1980. 2:1265–8.
Article2.Chaussy C., Schmiedt E., Jocham D., Brendel W., Forssmann B., Walther V. First clinical experience with extracorporeally induced destruction of kidney stones by shock waves. J Urol. 1982. 127:417–20.
Article3.Lackner H., Barton LJ. Cortical blood flow in ureteral obstruction. Invest Urol. 1970. 8:319–23.4.Jones DA., Atherton JC., O' Reilly PH., Barnard RJ., Georqe NJ. Assessment of the nephron segments involved in post-obstructive diuresis in man, using lithium clearance. Br J Urol. 1989. 64:559–63.
Article5.Gee WF., Kiviat MD. Ureteral response to partial obstruction. Smooth muscle hyperplasia and connective tissue proliferation. Invest Urol. 1975. 12:309–16.6.Netto Junior NR., Claro JF., Lemos GC., Cortado PL. Treatment options for ureteral calculi: endourology or extracorporeal shock wave lithotripsy. J Urol. 1991. 146:5–7.7.Ozgur S., Erol A., Gunes Z., Dalva I., Cetin S. Predictive value of a new scoring system for the outcome of primary in situ experimental extracorporeal shock wave lithotripsy of upper ureteral calculi. Eur Urol. 1995. 28:36–9.8.Seitz C., Fajkovic H., Waldert M., Tanovic E., Remzi M., Kramer G, et al. Extracorporeal shock wave lithotripsy in the treatment of proximal ureteral stones: Does the presence and degree of hydronephrosis affect success? Eur Urol. 2006. 49:378–83.
Article9.Cietak KA., Newton JR. Serial qualitative maternal nephrosonography in pregnancy. Br J Radiol. 1985. 58:399–404.
Article10.Segura JW., Preminger GM., Assimos DG., Dretler SP., Kahn RI., Lingeman JE, et al. Ureteral stones clinical guidelines panel summary report on the management of ureteral calculi. J Urol. 1997. 158:1915–21.
Article11.Ueno A., Kawamura T., Ogawa A., Takayasu H. Relation of spontaneous passage of ureteral calculi to size. Urology. 1977. 10:544–6.
Article12.Tiselius HG., Ackermann D., Aiken P., Buck C., Conort P., Gallucci M. Guidelines on urolidiiasis. Eur Urol. 2001. 40:362–71.13.Newman DM., Lingeman JE. Management of upper urinary calculi with extracorporeal shockwave lithotripsy. Compr Ther. 1989. 15:35–40.14.Dretler SP. Ureteral stone disease. Options for management. Urol Clin North Am. 1990. 17:217–30.15.Miller K., Bubeck JR., Hautmann R. Extracorporeal shockwave lidiotripsy of distal ureteral calculi. Eur Urol. 1986. 12:305–7.16.Kwon DD., Park KS., Min BK. The result of primary in situ extracorporeal shock wave lithotripsy for ureteral stones. Korean J Urol. 1992. 33:266–71.17.Kim HH., Lee JH., Park EC., Byeon SS., Oh SJ., Paick JS, et al. In situ extracorporeal shock wave lithotripsy for ureteral calculi: investigation of the factors influencing on stone fragmentation and the appropriate session for changing treatment modality. Korean J Urol. 1995. 36:722–30.18.Miller OF., Kane CJ. Time to stone passage for observed ureteral calculi: a guide for patient education. J Urol. 1999. 162:688–90.
Article19.Coll D., Varanelli M., Smith RC. Relations hip of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. AJR Am J Roentgenol. 2002. 178:101–3.20.Sinha M., Kekre NS., Chacko KN., Devasia A., Lionel G., Pandey AP, et al. Does failure to visualize the ureter distal to an impacted calculus constitute an impediment to successful lithotripsy? J Endourol. 2004. 18:431–5.
Article21.Morse RM., Resnick MI. Ureteral calculi: natural history and treatment in an era of advanced technology. J Urol. 1991. 145:263–5.
Article22.Singh I., Gupta NP., Hemal AK., Dogra PN., Ansari MS., Seth A, et al. Impact of power index, hydroureteronephrosis, stone size, and composition on the efficacy of in situ boosted ESWL for primary proximal ureteral calculi. Urology. 2001. 58:16–22.
Article23.Demirbas M., Kose AC., Samli M., Guler C., Kara T., Karalar M. Extracorporeal shock wave lithotripsy for solitary distal urinary stones: Does the degree of ureteral obstruction affect success? J Endourol. 2004. 18:237–40.24.Kim HH., Lee JH., Park MS., Lee SE., Kim SW. In situ extracorporeal shockwave lithotripsy for ureteral calculi: investigation of factors influencing stone fragmentation and appropriate number of sessions for changing treatment modality. J Endourol. 1996. 10:501–5.
Article25.Kageyama S., Hirai S., Higashi Y. An investigation of factors associated with failure of extracorporeal shock wave lithotripsy for ureteral calculi. Hinyokika Kiyo. 2000. 46:371–6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical experience of ureteral stones by extracorporeal shock wave lithotripsy
- Extracorporeal shock wave lithotripsy of ureteral stones : Investigation of the factors influencing upon stone fragmentation
- The Effect of Tamsulosin on Expulsion of Ureteral Stones after Extracorporeal Shock Wave Lithotripsy
- Clinical Experience of Extracorporeal Shock Wave Lithotripsy for Urinary Calculi
- Comparison between Rigid Ureteroscopic Stone Removal (URS) and Extracorporeal Shock Wave Lithotripsy (ESWL) for Large (>10mm) Upper Ureteral Stones
