Basic principles and applications of 18F-FDG-PET/CT in oral and maxillofacial imaging: A pictorial essay
- Affiliations
-
- 1Department of Oral Diagnosis and Polyclinics, Faculty of Dentistry, The Hong Kong University, Hong Kong. jellodent@yahoo.com
- 2BeamReaders Inc., Orlando, FL, USA.
- 3Departments of Otolaryngology and Radiology, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA.
- KMID: 1974503
- DOI: http://doi.org/10.5624/isd.2014.44.4.325
Abstract
- A combination of positron emission tomography (PET) with 18F-labeled fluoro-2-deoxyglucose (18F-FDG) and computed tomography (18F-FDG-PET/CT) has increasingly become a widely used imaging modality for the diagnosis and management of head and neck cancer. On the basis of both recent literature and our professional experience, we present a set of principles with pictorial illustrations and clinical applications of FDG-PET/CT in the evaluation and management planning of squamous cell carcinoma of the oral cavity and oropharynx. We feel that this paper will be of interest and will aid the learning of oral and maxillofacial radiology trainees and practitioners.
MeSH Terms
Figure
-

Fig. 1 Annihilation coincidence detection (ACD). When a positron is emitted by a nuclear transformation, it scatters through matter losing energy and annihilates with an electron, resulting in two 511-keV photons that are emitted in nearly opposite directions (left). When two interactions are simultaneously detected within a ring of detectors surrounding the patient (right), it is assumed that annihilation occurred on the line connecting the interactions (line of response, LOR). ACD acts as a collimator for the positron emission tomography (PET) scanner (electronic collimation) by determining the path of the detected photons.
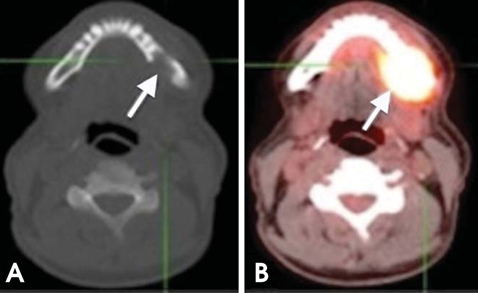
Fig. 2 A 64-year-old man with T4 squamous cell carcinoma (SCC) of the lingual gingiva of the left posterior mandible. (A) Axial plain computed tomography (CT) image shows bone destruction of the left posterior mandible (arrow). (B) Axial PET/CT scan shows intense fluoro-2-deoxyglucose (FDG) uptake in the same area (arrow).
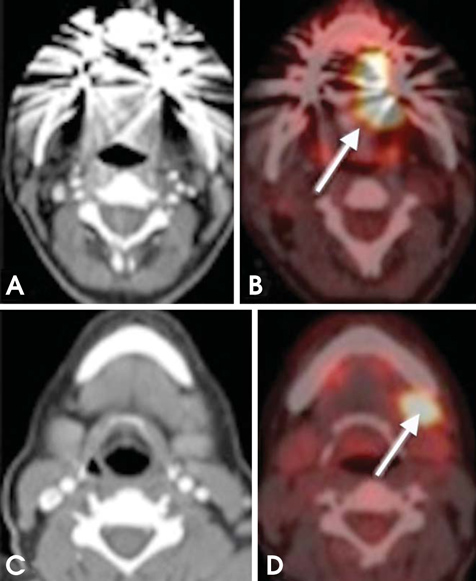
Fig. 3 A 56-year-old man diagnosed with SCC of the lateral border of the tongue (left side). (A, B) Axial CT and PET/CT images reveal increased FDG uptake in the lateral border of the tongue (arrow). (C, D) Axial CT and PET/CT images at a lower level show increased uptake in a left level IB lymph node (arrow).

Fig. 4 False-negative CT overlooks nodal disease. A 57-year-old man diagnosed with Hodgkin's lymphoma. (A) Non-enhanced CT scan showed normal study. The lymph nodes are normal according to radiographic criteria. However, the fused PET/CT images (B) show many pathologic nodes surrounding the paraspinal musculature.
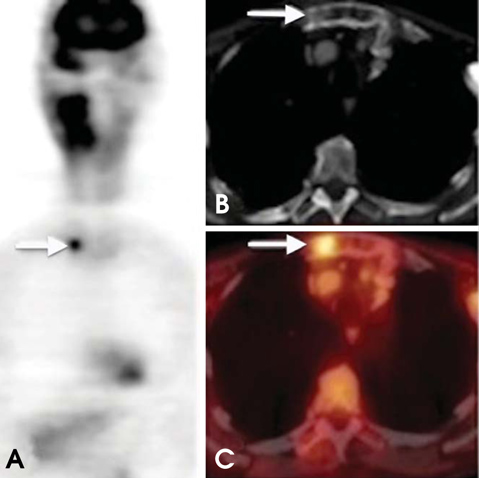
Fig. 5 Metastatic head and neck SCC (HNSCC). A 61-year-old male with T3 SCC of the right tosillar fossa. Whole-body PET shows a focus of increased uptake (arrow) in the sternum, which proved to be a distant metastasis. The CT component is still needed to adequately assess lesion location. PET/CT is useful for detecting distant metastasis in patients undergoing restaging or surveillance.
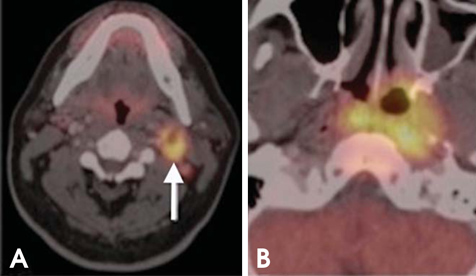
Fig. 6 Unknown primary tumor. A 54-year-old patient presented with an enlarging left neck mass. (A) CT shows a level IIA lymph node (arrow); fine-needle aspiration biopsy showed metastatic squamous cell carcinoma. CT chest and panendoscopy failed to disclose the primary tumor. (B) PET/CT shows the patient's primary tumor in the nasopharynx.
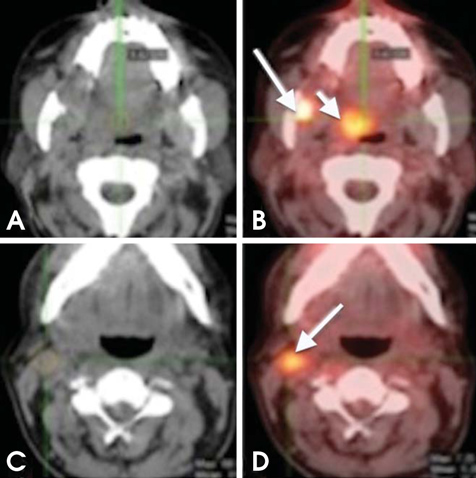
Fig. 7 Synchronous tumor. A 65-year-old man recently diagnosed with SCC of the right mandibular retromolar trigon. (A, B) Axial CT and PET/CT images show intense FDG uptake in the retromolar trigon; another focal area of increased uptake can be seen in the right soft palate (short arrow); further biopsy confirmed a tumor (metachronous). (C, D) Axial CT and PET/CT images show increased FDG uptake in a right level IIA lymph node (arrow).
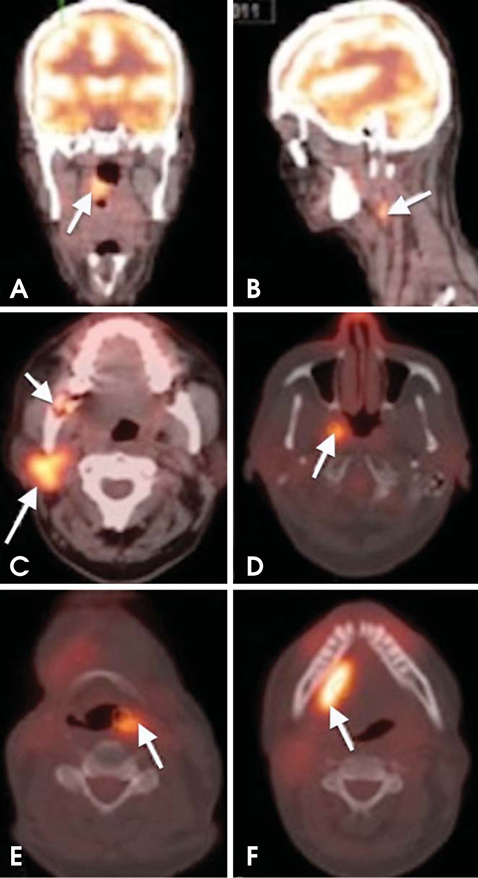
Fig. 8 Metachronous tumors. A 64-year-old woman diagnosed with SCC of the right tonsillar fossa. (A, B) Axial PET/CT images show increased FDG uptake in the right tonsillar fossa and ipsilateral level IIA level nodal metastasis. (C, D) Surveillance PET/CT scan performed 10 months after chemoradiation demonstrates new tumors in the right parotid gland and right lateral wall of the nasopharynx. The right retromolar trigon shows bone destruction with slightly increased metabolic activity of maximum standardized uptake value (SUVmax) of 5.68. This area represented radiation-induced osteomyelitis (short arrow in C). (E, F) The PET/CT scan performed 9 months later reveals additional metachronous tumors in the left piriform fossa and right floor of the mouth.

Fig. 9 Monitoring therapy response. Nasopharyngeal carcinoma with ipsilateral level IIB nodal metastasis. (A, C) Axial PET/CT images show increased FDG uptake in the right nasopharynx and ipsilateral level IIB lymph nodes. (B, D) Six months after initiation of chemoradiation, complete anatomic and metabolic response to treatment.

Fig. 10 Coronal PET images show diffuse whole-body muscle uptake of FDG. This condition can be caused by insulin, recent food intake, and strenuous exercise that involves many muscle groups.
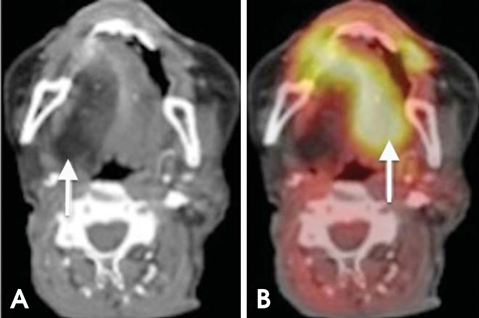
Fig. 11 XII nerve dysfunction. (A) Axial CT image shows fatty degeneration of the right half of the tongue. (B) PET/CT shows increased FDG avidity in the left (normal) half of the tongue (paradoxical finding).
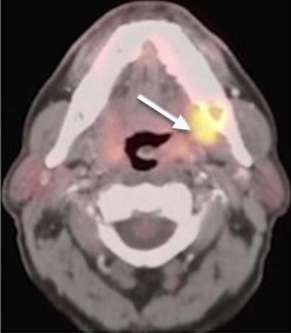
Fig. 12 A 51-year-old man with a 3-year history of nasopharyngeal carcinoma. The patient presented with new mucosal swelling in the left retromolar trigon; recurrence was suspected. PET-CT image shows increased metabolism in the corresponding area (arrow); however, further clinical examination and biopsy revealed a dental abscess.

Fig. 13 False-negative PET/CT overlooks nodal metastasis. (A) On axial PET/CT, the lymph node (arrow) has low FDG uptake belying nodal disease. (B) On axial contrast-enhanced CT, the central necrosis and rounded configuration are clues to the nodal metastasis; confirmed with further biopsies. A PET/CT examination of such conditions may yield false-negative findings (metastatic thyroid carcinoma).
Reference
-
1. Chandra R. Nuclear medicine physics: the basics. 6th ed. Philadelphia: Lippincott Williams & Wilkins;2004.2. Blodgett TM, Fukui MB, Snyderman CH, Branstetter BF 4th, McCook BM, Townsend DW, et al. Combined PET-CT in the head and neck: part 1. Physiologic, altered physiologic, and artifactual FDG uptake. Radiographics. 2005; 25:897–912.3. Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006; 56:106–130.
Article4. Forastiere A, Koch W, Trotti A, Sidransky D. Head and neck cancer. N Engl J Med. 2001; 345:1890–1900.
Article5. Antoch G, Vogt FM, Freudenberg LS, Nazaradeh F, Goehde SC, Barkhausen J, et al. Whole-body dual-modality PET/CT and whole-body MRI for tumor staging in oncology. JAMA. 2003; 290:3199–3206.
Article6. Ha PK, Hdeib A, Goldenberg D, Jacene H, Patel P, Koch W, et al. The role of positron emission tomography and computed tomography fusion in the management of early-stage and advanced-stage primary head and neck squamous cell carcinoma. Arch Otolaryngol Head Neck Surg. 2006; 132:12–16.
Article7. Suzuki H, Hasegawa Y, Terada A, Ogawa T, Hyodo I, Suzuki M, et al. Limitations of FDG-PET and FDG-PET with computed tomography for detecting synchronous cancer in pharyngeal cancer. Arch Otolaryngol Head Neck Surg. 2008; 134:1191–1195.
Article8. Branstetter BF 4th, Blodgett TM, Zimmer LA, Snyderman CH, Johnson JT, Raman S, et al. Head and neck malignancy: Is PET/CT more accurate than PET or CT alone? Radiology. 2005; 235:580–586.
Article9. Yau YY, Samman N, Yeung RW. Positron emission tomography/computed tomography true fusion imaging in clinical head and neck oncology: early experience. J Oral Maxillofac Surg. 2005; 63:479–486.10. Layland MK, Sessions DG, Lenox J. The influence of lymph node metastasis in the treatment of squamous cell carcinoma of the oral cavity, oropharynx, larynx, and hypopharynx: N0 versus N+. Laryngoscope. 2005; 115:629–639.
Article11. McHam SA, Adelstein DJ, Rybicki LA, Lavertu P, Esclamado RM, Wood BG, et al. Who merits a neck dissection after definitive chemoradiotherapy for N2-N3 squamous cell head and neck cancer? Head Neck. 2003; 25:791–798.
Article12. Brouwer J, Senft A, de Bree R, Comans EF, Golding RP, Castelijns JA, et al. Screening for distant metastases in patients with head and neck cancer: is there a role for (18)FDG-PET? Oral Oncol. 2006; 42:275–280.
Article13. Jones J, Farag I, Hain SF, McGurk M. Positron emission tomography (PET) in the management of oro-pharyngeal cancer. Eur J Surg Oncol. 2005; 31:170–176.
Article14. Ng SH, Yen TC, Liao CT, Chang JT, Chan SC, Ko SF, et al. 18F-FDG PET and CT/MRI in oral cavity squamous cell carcinoma: a prospective study of 124 patients with histologic correlation. J Nucl Med. 2005; 46:1136–1143.15. Krabbe CA, Dijkstra PU, Pruim J, van der Laan BF, van der Wal JE, Gravendeel JP, et al. FDG PET in oral and oropharyngeal cancer. Value for confirmation of N0 neck and detection of occult metastases. Oral Oncol. 2008; 44:31–36.
Article16. Kim MR, Roh JL, Kim JS, Choi SH, Nam SY, Kim SY. 18F-fluorodeoxyglucose-positron emission tomography and bone scintigraphy for detecting bone metastases in patients with malignancies of the upper aerodigestive tract. Oral Oncol. 2008; 44:148–152.
Article17. Kwee TC, Kwee RM. Combined FDG-PET/CT for the detection of unknown primary tumors: systematic review and metaanalysis. Eur Radiol. 2009; 19:731–744.
Article18. Freudenberg LS, Fischer M, Antoch G, Jentzen W, Gutzeit A, Rosenbaum SJ, et al. Dual modality of 18F-fluorodeoxyglucose-positron emission tomography/computed tomography in patients with cervical carcinoma of unknown primary. Med Princ Pract. 2005; 14:155–160.19. Torizuka T, Tanizaki Y, Kanno T, Futatsubashi M, Naitou K, Ueda Y, et al. Prognostic value of 18F-FDG PET in patients with head and neck squamous cell cancer. AJR Am J Roentgenol. 2009; 192:W156–W160.20. Machtay M, Natwa M, Andrel J, Hyslop T, Anne PR, Lavarino J, et al. Pretreatment FDG-PET standardized uptake value as a prognostic factor for outcome in head and neck cancer. Head Neck. 2009; 31:195–201.
Article21. Allal AS, Slosman DO, Kebdani T, Allaoua M, Lehmann W, Dulguerov P. Prediction of outcome in head-and-neck cancer patients using the standardized uptake value of 2-[18F]fluoro-2-deoxy-D-glucose. Int J Radiat Oncol Biol Phys. 2004; 59:1295–1300.
Article22. Yao M, Smith RB, Graham MM, Hoffman HT, Tan H, Funk GF, et al. The role of FDG PET in management of neck metastasis from head-and-neck cancer after definitive radiation treatment. Int J Radiat Oncol Biol Phys. 2005; 63:991–999.
Article23. de Visscher AV, Manni JJ. Routine long-term follow-up in patients treated with curative intent for squamous cell carcinoma of the larynx, pharynx, and oral cavity. Does it make sense? Arch Otolaryngol Head Neck Surg. 1994; 120:934–939.
Article24. Porceddu SV, Jarmolowski E, Hicks RJ, Ware R, Weih L, Rischin D, et al. Utility of positron emission tomography for the detection of disease in residual neck nodes after (chemo) radiotherapy in head and neck cancer. Head Neck. 2005; 27:175–181.25. Zimmer LA, Snyderman C, Fukui MB, Blodgett T, McCook B, Townsend DW, et al. The use of combined PET/CT for localizing recurrent head and neck cancer: the Pittsburgh experience. Ear Nose Throat J. 2005; 84:104106108–110.
Article26. Goerres GW, Schmid DT, Grätz KW, von Schulthess GK, Eyrich GK. Impact of whole body positron emission tomography on initial staging and therapy in patients with squamous cell carcinoma of the oral cavity. Oral Oncol. 2003; 39:547–551.
Article27. Ryan WR, Fee WE Jr, Le QT, Pinto HA. Positron emission tomography for surveillance of head and neck cancer. Laryngoscope. 2005; 115:645–650.28. Fukui MB, Blodgett TM, Snyderman CH, Johnson JJ, Myers EN, Townsend DW, et al. Combined PET-CT in the head and neck. Part 2. Diagnostic uses and pitfalls of oncologic imaging. Radiographics. 2005; 25:913–930.29. Kubota R, Yamada S, Kubota K, Ishiwata K, Tamahashi N, Ido T. Intratumoral distribution of fluorine-18-fluorodeoxyglucose in vivo: high accumulation in macrophages and granulation tissues studied by microautoradiography. J Nucl Med. 1992; 33:1972–1980.30. Veeramachaneni R, Gulick J, Halldorsson A, Van T, Zhang P, Herrera G. Benign myoepithelioma of the lung: a case report and review of the literature. Arch Pathol Lab Med. 2001; 125:1494–1496.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Use of 18F-FDG PET/CT in Second Primary Cancer
- Esophageal Leiomyoma with intense FDG uptake on 18F-FDG PET/CT
- Nodular Fasciitis Mimicking Malignant Tumor on 18F-FDG PET/CT
- Uptake of 18F-FDG in the Angioleiomyoma of the Leg
- Recurrent Follicular Dendritic Cell Sarcoma of the Parotid Gland Imaged with 18F-FDG PET/CT
