Reconstruction of the Orbit With a Temporalis Muscle Flap After Orbital Exenteration
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Okmeydani Training and Reseach Hospital, Istanbul, Turkey. tolgins@hotmail.com
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Meram University School of Medicine, Konya, Turkey.
- KMID: 1973488
- DOI: http://doi.org/10.3342/ceo.2015.8.1.52
Abstract
OBJECTIVES
This study presents the role of the temporalis muscle flap in primary reconstruction after orbital exenteration.
METHODS
A retrospective nonrandomized study of orbital exenterations performed between 1990 and 2010 for malignant tumors of the skin, paranasal sinus, and nasal cavity is presented.
RESULTS
The study included 13 patients (nine men, four women; age range, 30-82 years) with paranasal sinus, nasal cavity, or skin carcinomas. Primary reconstruction of the cavity was performed in all patients after orbital exenteration. No visible defects in the muscle flap donor site were present. Local recurrences were readily followed up with nasal endoscopy, whereas radiology helped to diagnose intracranial involvement in three patients. Two patients died of systemic metastases and five died for other reasons
CONCLUSION
The temporalis muscle flap is readily used to close the defect after orbital exenteration, and does not prevent the detection of recurrence.
Keyword
MeSH Terms
Figure
-
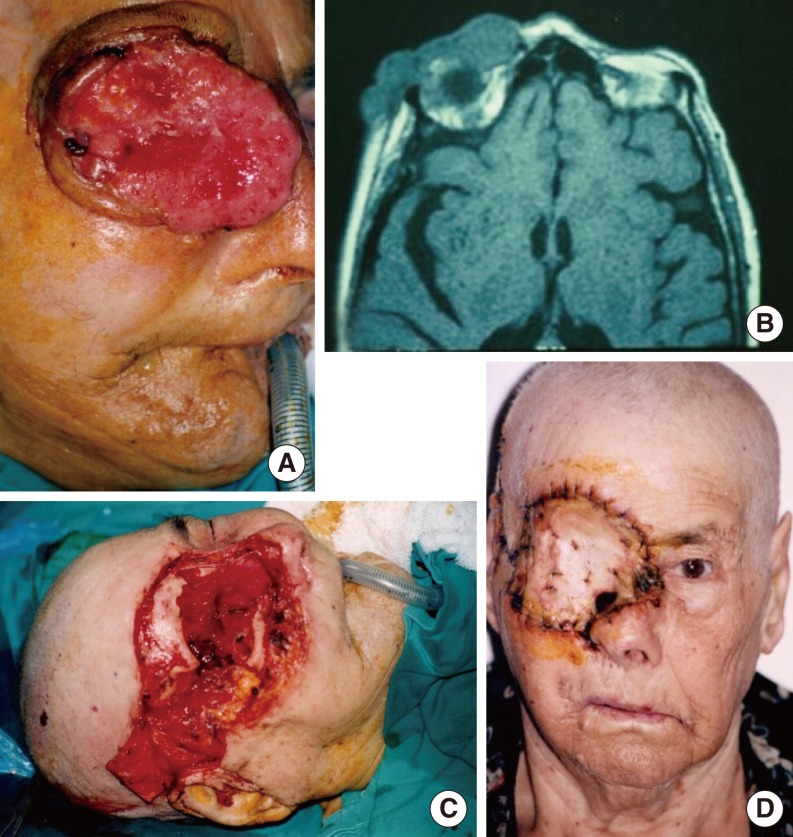
Fig. 1 A 65-year-old man with a malignant tumor invading the orbit. (A) Preoperative photography of the exophytic malignant tumor, which invades the eye and the orbit. (B) The axial magnetic resonance imaging scans were interpreted as solid, irregular enhancement invading the eye and orbit. (C) Intraoperative operative technique of the orbital exenteration of the eye. (D) Postoperative temporalis muscle flap closure with full-thickness skin graft.
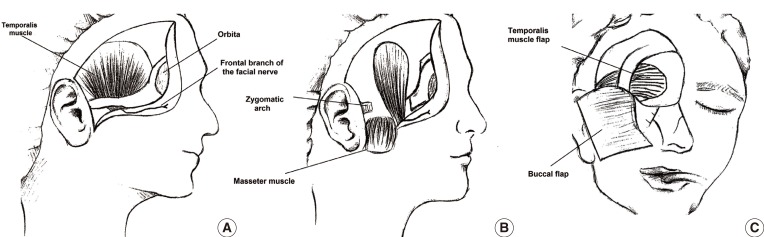
Fig. 2 The surgical technique. (A) The temporoparietal fascia is elevated with a skin flap. The zygomatic arch and lateral orbital wall of the outer surface are exposed. (B) An osteotomy is made in the zygomatic arch and the temporalis muscle flap is elevated from the junction of the perichondrium subperiosteally. (C) A tunnel is created by drilling in the lateral orbital wall, and the flap is laid down.

Fig. 3 A 54-year-old woman with squamous cell carcinoma in the ethmoid sinus invading the left orbit. (A) Preoperative photography of the patient with proptosis in the left eye. (B) The axial computed tomography scans were interpreted as a solid mass in the etmoid air cells invading the nasal septum, left lamina papyracea and left optic nerve. (C) Intraoperative operative technique of the tunnel created to ensure the passage of the temporalis muscle flap to the orbit. (D) Postoperative temporalis muscle flap closure with the eyelid skin.
Reference
-
1. Kennedy RE. Indications and surgical techniques for orbital exenteration. Ophthalmology. 1979; 5. 86(5):967–973. PMID: 397452.
Article2. Rose GE, Wright JE. Exenteration for benign orbital disease. Br J Ophthalmol. 1994; 1. 78(1):14–18. PMID: 8110691.
Article3. Hargrove RN, Wesley RE, Klippenstein KA, Fleming JC, Haik BG. Indications for orbital exenteration in mucormycosis. Ophthal Plast Reconstr Surg. 2006; Jul-Aug. 22(4):286–291.
Article4. Cook BE Jr, Bartley GB. Treatment options and future prospects for the management of eyelid malignancies: an evidence-based update. Ophthalmology. 2001; 11. 108(11):2088–2098. PMID: 11713084.
Article5. Rahman I, Cook AE, Leatherbarrow B. Orbital exenteration: a 13 year Manchester experience. Br J Ophthalmol. 2005; 10. 89(10):1335–1340. PMID: 16170127.
Article6. Nassab RS, Thomas SS, Murray D. Orbital exenteration for advanced periorbital skin cancers: 20 years experience. J Plast Reconstr Aesthet Surg. 2007; 60(10):1103–1109. PMID: 17434350.
Article7. Hussain A, Murthy P, Silver SM. Pedicled temporoparietal galeal myofascial flap for orbital and cheek lining following radical maxillectomy. Rhinology. 1996; 12. 34(4):227–231. PMID: 9050102.8. Cuesta-Gil M, Concejo C, Acero J, Navarro-Vila C, Ochandiano S. Repair of large orbito-cutaneous defects by combining two classical flaps. J Craniomaxillofac Surg. 2004; 2. 32(1):21–27. PMID: 14729046.
Article9. Roche P, Timon C. Orbital exenteration in periorbital malignancies. Surgeon. 2012; 8. 10(4):189–193. PMID: 22818275.
Article10. Ben Simon GJ, Schwarcz RM, Douglas R, Fiaschetti D, McCann JD, Goldberg RA. Orbital exenteration: one size does not fit all. Am J Ophthalmol. 2005; 1. 139(1):11–17. PMID: 15652823.11. Guerra AS, Barbosa R, Choupina M, Pinho C, Ribeiro M, Pontes L. Orbital exenteration for eyelid skin carcinoma. Eur J Plast Surg. 2011; 8. 34(4):239–243.
Article12. Serrano NA, Trenite GN, Yueh B, Farwell DG, Futran ND, Mendez E. Risk factors associated with repair of orbital and lateral skull defects. Arch Facial Plast Surg. 2012; Mar-Apr. 14(2):97–103. PMID: 22183060.
Article13. Howard DJ, Lund VJ, Wei WI. Craniofacial resection for tumors of the nasal cavity and paranasal sinuses: a 25-year experience. Head Neck. 2006; 10. 28(10):867–873. PMID: 16823871.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rectus Abdominis Free Flap Reconstruction for Orbital-Maxillary Defect in Advanced Maxillary Sinus Cancer
- Orbital Reconstruction with Free Flaps after Orbital Exenteration
- Extended temporalis flap for skull base reconstruction
- Patient-specific PEEK implants for immediate restoration of temporal fossa after maxillary reconstruction with temporalis muscle flap
- Reconstruction of the Orbital Wall with the Galeal- frontalis-pericranial-calvarial Bone Flap
