Tuberc Respir Dis.
2006 Sep;61(3):227-232. 10.4046/trd.2006.61.3.227.
The Complementary Role of FEV6 in Bronchodilator Reversibility Test for the Old Age
- Affiliations
-
- 1Department of Internal Medicine, Eulji University School of Medicine, Daejeon, Korea. lydmd@hanmail.net
- KMID: 1970261
- DOI: http://doi.org/10.4046/trd.2006.61.3.227
Abstract
-
BACKGROUND: In the measurement of bronchodilator reversibility, the forced expiratory volume in one second(FEV(1)) and the forced vital capacity(FVC) are commonly used parameters and recommended criteria for the reversibility requiring an increase of more than 200ml and 12% above the baseline, respectively. However, aged patients do not often meet the criteria of an increase in volume(>200ml) even though the medical history of that patient is adequate for asthma. This study investigated the role of the forced expiratory volume in six seconds(FEV(6)) in the bronchodilator reversibility test in elderly patients.
METHODS
A total of 236 patients more than 65 years of age with a FEV(1)/FVC ratio<80% were enrolled in this study. The bronchodilator revesibility tests were examined. With the setting FEV(1) as the baseline, the patients were divided into three groups; Group I: FEV(1)> or = 80% of the predicted value, Group II: 60%
Positive reversibility in the FEV(1), FEV(6), and FVC was in 33(14.0%), 49(20.8%) and 55(23.3%). However, Group III presented with reversibility in the FEV(1), FEV(6), and FVC in 15(22.4%), 30(44.8%) and 32(47.8%) respectively.
CONCLUSIONS
The FEV6 might be used as a complementary parameter in bronchodilatror reversibility in elderly patients. However, more study will be needed to determine the usefulness of FEV(6) in bronchodilator reversibility test.
MeSH Terms
Figure
-
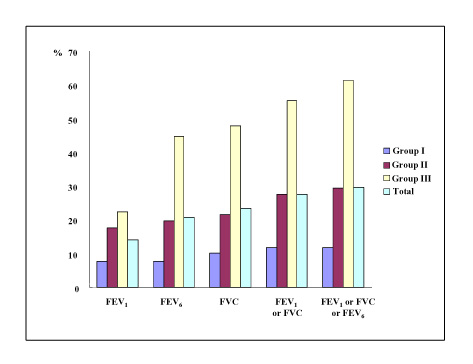
Figure 1 Positive reversibility according to the different parameters for each groups of 236 patients
Reference
-
1. Killian KJ, Summers E, Watson RM, O'Byrne PM, Jones NL, Campbell EJ. Factors contributing to dyspnoea during bronchoconstriction and exercise in asthmatic subjects. Eur Respir J. 1993. 6:1004–1010.2. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005. 26:319–338.3. Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005. 26:948–968.4. Stoller JK, Buist AS, Burrows B, Crystal RG, Fallat RJ, McCarthy K, et al. Quality control of spirometry testing in the registry for patients with severe alpha1-antitrypsin deficiency: alpha1-Antitrypsin Deficiency Registry Study Group. Chest. 1997. 111:899–909.5. Eaton T, Withy S, Garrett JE, Mercer J, Whitlock RM, Rea HH. Spirometry in primary care practice: the importance of quality assurance and the impact of spirometry workshops. Chest. 1999. 116:416–423.6. Swanney MP, Beckert LE, Frampton CM, Wallace LA, Jensen RL, Crapo RO. Validity of the American Thoracic Society and other spirometric algorithms using FVC and forced expiratory volume at 6 s for predicting a reduced total lung capacity. Chest. 2004. 126:1861–1866.7. Akpinar-Elci M, Fedan KB, Enright PL. FEV6 as a surrogate for FVC in detecting airways obstruction and restriction in the workplace. Eur Respir J. 2006. 27:374–377.8. American Thoracic Society. Standardization of Spirometry, 1994 update. Am J Respir Crit Care Med. 1995. 152:1107–1136.9. Pellegrino R, Rodarte JR, Brusasco V. Assessing the reversibility of airway obstruction. Chest. 1998. 114:1607–1612.10. Lorber DB, Kaltenborn W, Burrows B. Responses to isoproterenol in a general population sample. Am Rev Respir Dis. 1978. 118:855–861.11. Dales RE, Spitzer WO, Tousignant P, Schechter M, Suissa S. Clinical interpretation of airway response to a bronchodilator: epidemiologic considerations. Am Rev Respir Dis. 1988. 138:317–320.12. Anthonisen NR, Wright EC. Bronchodilator response in chronic obstructive pulmonary disease. Am Rev Respir Dis. 1986. 133:814–819.13. Sourk RL, Nugent KM. Bronchodilator testing: confidence intervals derived from placebo inhalations. Am Rev Respir Dis. 1983. 128:153–157.14. Enright RL, Connett JE, Bailey WC. The FEV1/FEV6 predicts lung function decline in adult smokers. Respir Med. 2002. 96:444–449.15. Vandevoorde J, Verbanck S, Schuermans D, Kartounian J, Vincken W. Obstructive and restrictive spirometric patterns: fixed cut-offs for FEV1/FEV6 and FEV6. Eur Respir J. 2006. 27:378–383.16. Demir T, Ikitimur HD, Koc N, Yildirim N. The role of FEV6 in the detection of airway obstruction. Respir Med. 2005. 99:103–106.17. Killian KJ, Watson R, Otis J, St Amand TA, O'Byrne PM. Symptom perception during acute bronchoconstriction. Am J Respir Crit Care Med. 2000. 162:490–496.18. Kendrick AH, Higgs CM, Whitfield MJ, Laszlo G. Accuracy of perception of severity of asthma: patients treated in general practice. BMJ. 1993. 307:422–424.19. Nowak RM, Pensler MI, Sarkar DD, Anderson JA, Kvale PA, Ortiz AE, et al. Comparison of peak expiratory flow and FEV1 admission criteria for acute bronchial asthma. Ann Emerg Med. 1982. 11:64–69.20. Dow L. Asthma in older people. Clin Exp Allergy. 1998. 28:195–202.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of Bronchodilator Reversibility Testing in Differentiating Asthma From COPD
- The Role of FEV6 in the Diagnosis of Obstructive Airway Disease for the Old Age
- The Time Responses of Spirometric Values in Response to Single Doses of Inhaled Salbutamol
- Clinical Usefulness of Impulse Oscillometry in Estimation of the Reversibility of Airway Obstruction in Adult Asthmatics
- Utility of Infant Pulmonary Function Test in Bronchopulmonary Dysplasia
