High-Resolution Computed Tomographic Findings of the Pneumoconiosis with p-Nodule
- Affiliations
-
- 1Department of Diagnostic Radiology, College of Medicine, Chungbuk National University, Cheongju, Korea. sjkim@chungbuk.ac.kr
- 2Occupational Lung Diseases Institute, COMWEL, Ansan, Korea.
- KMID: 1941770
- DOI: http://doi.org/10.3348/jksr.2014.70.6.423
Abstract
- PURPOSE
We describe high-resolution computed tomographic (HRCT) findings in type p pneumoconiosis.
MATERIALS AND METHODS
In total, 147 patients who were confirmed with pneumoconiosis on chest radiographs then underwent HRCT; 38 patients with p-nodules on chest radiographs constituted the study population. Chest CT findings, such as the appearance of the p-nodules (ill-defined small nodules, bi-branching structure, well-marginated micronodule, tree-in-bud appearance), the presence of subpleural nodules, changes in the bronchus (e.g., thickening of the bronchial wall, bronchiectasis), and presence of emphysema (centrilobular, perinodular) were reviewed retrospectively by two radiologists in consensus.
RESULTS
In the 38 patients, two did not have nodules, just emphysema. The majority of the p-nodules in the other 36 patients were located in the upper and middle lung fields (n = 33, 91.7%). The most common HRCT findings of p-nodules were ill-defined small nodules, larger than 1.5 mm, and with bi-branching structures (32/36, 88.9%). Well-marginated micronodules were also common (27/36, 75.0%); however, the tree-in-bud appearance was rare (4/36, 11.1%). Changes in the bronchus [thickening of the bronchial wall (27/36, 75.0%), bronchiectasis (19/36, 52.8%)] were identified in 29 patients (80.6%). Centrilobular emphysema and perinodular emphysema were seen in 19 (52.8%) and 9 (25.0%) patients, respectively. All of the patients with perinodular emphysema also had centrilobular emphysema. Subpleural nodules were identified in 17 patients (47.2%).
CONCLUSION
The distribution of p-nodules was predominantly upper and middle. The most common HRCT findings of p-nodules were ill-defined small nodules and bi-branching structures. Additional useful findings are well-marginated micronodules and changes in the bronchus, such as thickening of the bronchial wall and bronchiectasis.
MeSH Terms
Figure
-

Fig. 1 A 56-year-old man who previously worked as coal miner for 13 years and who had p/s, 1/0 pneumoconiosis. High-resolution CT scans show diffusely distributed, ill-defined small nodules (white arrow) and bi-branching structures (circle). The ill-defined small nodules are larger than the upper limit of p-nodule (1.5 mm). The subpleural nodules, so called pseudoplaque, are also seen in the right upper lobe (black arrow).

Fig. 2 A 63-year-old man who previously worked as coal miner for 21 years and who had p/q, 1/2 pneumoconiosis. High-resolution CT scans show well marginated micronodules (circle) which clustered together at middle lung zone on the sagittal plane. Some small round nodules corresponding to q- and r-nodule (arrows), and subpleural nodules are also seen in the right upper lobe.
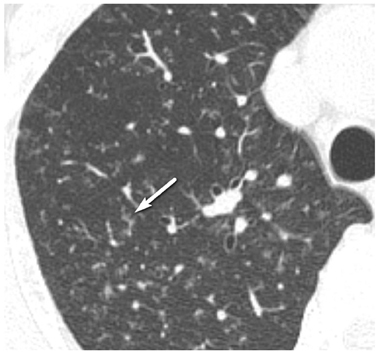
Fig. 3 A 61-year-old man who previously worked as coal miner for 16 years and who had p/s, 1/0 pneumoconiosis. High-resolution CT scan shows tree-in-bud appearance (arrow) in the right upper lobe. Also, ill-defined small nodules and bi-branching structures are seen.

Fig. 4 High-resolution CT scan of 69-year-old man who previously worked as coal miner for 15 years shows dilatation of the peripheral bronchus (circle) and thickening of the bronchial wall (arrow).

Fig. 5 A 61-year-old man who previously worked as coal miner for 26 years and who had p/s, 1/1 pneumoconiosis. High-resolution CT scan shows numerous small areas of low attenuation. Some of these areas had prominent central (arrow) or periphral dots (circle). Centrilobular and paraseptal emphysema in the right upper lobe were also seen.
Reference
-
1. International Labour Office. ILO international classification of radiographs of pneumoconiosis. Geneva: ILO Publications;1980.2. Gough I, James WRL, Wentworth JE. Comparison of radiological and pathological changes in coal workers' pneumoconiosis. J Fac Radiol (Lond). 1949; 1:28–23.3. Ryder R, Lyons JP, Campbell H, Gough J. Emphysema in coal workers' pneumoconiosis. Br Med J. 1970; 3:481–487.4. Seaton A, Lapp NL, Morgan WK. Relationship of pulmonary impairment in simple coal workers' pneumoconiosis to type of radiographic opacity. Br J Ind Med. 1972; 29:50–55.5. Akira M, Higashihara T, Yokoyama K, Yamamoto S, Kita N, Morimoto S, et al. Radiographic type p pneumoconiosis: high-resolution CT. Radiology. 1989; 171:117–123.6. Okada F, Ando Y, Yoshitake S, Ono A, Tanoue S, Matsumoto S, et al. Clinical/pathologic correlations in 553 patients with primary centrilobular findings on high-resolution CT scan of the thorax. Chest. 2007; 132:1939–1948.7. Collins J, Stern EJ, Franquet TC. Bronchiolar disease: a spectrum of causes and CT findings. Appl Radiol. 2002; 31:20–28.8. Hansell DM. Small airways diseases: detection and insights with computed tomography. Eur Respir J. 2001; 17:1294–1313.9. Hirakata K. [Pathologic-HRCT correlation of pneumoconiosis--a study on inflation-fixed lungs]. Nihon Igaku Hoshasen Gakkai Zasshi. 1992; 52:35–51.10. Yamane K. [Clinical study of pneumoconiosis featuring small nodules and without large opacities on high-resolution CT]. Nihon Igaku Hoshasen Gakkai Zasshi. 1996; 56:288–293.11. Duguid JB, Lambert MW. The pathogenesis of coal miner's pneumoconiosis. J Pathol Bacteriol. 1964; 88:389–403.12. Naidich DP, McCauley DI, Khouri NF, Stitik FP, Siegelman SS. Computed tomography of bronchiectasis. J Comput Assist Tomogr. 1982; 6:437–444.13. Bergin CJ, Müller NL, Vedal S, Chan-Yeung M. CT in silicosis: correlation with plain films and pulmonary function tests. AJR Am J Roentgenol. 1986; 146:477–483.14. Remy-Jardin M, Remy J, Farre I, Marquette CH. Computed tomographic evaluation of silicosis and coal workers' pneumoconiosis. Radiol Clin North Am. 1992; 30:1155–1176.15. Gough J. Emphysema in relation to pneumoconiosis. In : Proceedings of the Pneumoconiosis Conference, Johannesburg, 1959; Boston, MA: Little, Brown;1960. p. 200–204.16. Collins LC, Willing S, Bretz R, Harty M, Lane E, Anderson WH. High-resolution CT in simple coal workers' pneumoconiosis. Lack of correlation with pulmonary function tests and arterial blood gas values. Chest. 1993; 104:1156–1116.17. Diederich S, Lenzen H, Windmann R, Puskas Z, Yelbuz TM, Henneken S, et al. Pulmonary nodules: experimental and clinical studies at low-dose CT. Radiology. 1999; 213:289–298.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- HRCT findings of disseminated small nodular shadow in plain chest X-ray
- Comparison of Radiological Methods for the Study and Diagnosis of Pneumoconiosis: Simple Radiography and Computed Tomography
- High-resolution CT Findings of Welders' Pneumoconiosis
- The Diagnostic Role of HRCT in Simple Pneumoconiosis
- A Study on the Early Diagnosis of Pneumoconiosis
