The Usefulness of Sagittal Reformation for Diagnosis of Sternal Fracture
- Affiliations
-
- 1Department of Radiology, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea. andrew0668@hanmail.net
- KMID: 1897256
- DOI: http://doi.org/10.3348/jksr.2014.70.1.25
Abstract
- PURPOSE
The purpose of our study was to evaluate the usefulness of sagittal reformation of chest computed tomography for the diagnosis of sternal fracture after trauma.
MATERIALS AND METHODS
We retrospectively reviewed medical records and chest computer tomography (CT) of 716 patients in the emergency department after trauma between January and December 2010. Two radiologists investigated chest CT images. We investigated numbers and locations of sternal fractures on axial images only and on both axial and sagittal images for each radiologist.
RESULTS
First, radiologist found sternal fractures in 58 patients (70.7%) on only axial images, and 80 (97.5%) on both axial and sagittal images. Second, radiologist found fractures in 67 patients (81.7%) on axial image only and 81 (98.7%) on both axial and sagittal images. The sensitivity increased after adding sagittal reformation images for each radiologist (p < 0.05, respectively). On the axial images, the interobserver agreement was low (kappa = 0.596) between the two radiologists. However, on both axial and sagittal images, the interobserver agreement increased (kappa = 0.872).
CONCLUSION
Sagittal reformation of chest CT increases the chance of diagnosis for sternal fracture and leads to early diagnosis resulting in appropriate treatment.
MeSH Terms
Figure
-

Fig. 1 The patient with traffic accident. A. With axial images, two radiologists did not find any abnormality of sternum. B. With sagittal reformation images, they found cortical disruption in anterior aspect of mid sternal body (white arrow). C. Bone scan after 2 weeks, there was radioactivity in sternal body (white arrow). And there were some activities in Rt. 5th, Lt. 3-4th ribs due to multiple rib fractures (black arrowheads).
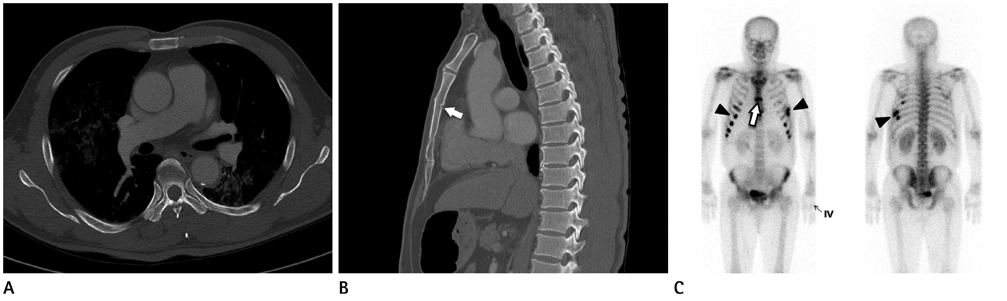
Fig. 2 The patient with traffic accident. A. With axial images, two radiologists did not find any abnormality of sternum. B. With sagittal reformation images, they found cortical disruption in posterior aspect of mid sternal body (white arrow). C. Bone scan after 2 weeks, there was radioactivity in sternal body (white arrow). And there were some activities in Rt. 4-9th, Lt. 6-9th ribs due to multiple rib fractures (black arrowheads).
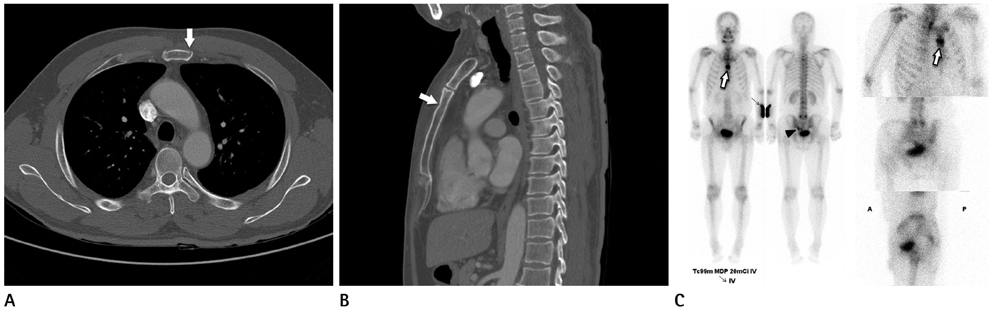
Fig. 3 The patient with fall down injury. A. With axial images, first radiologists did not find any abnormality of sternum, but second radiologist found cortical disruption in anterior aspect of mid sternal body (white arrow). B. With sagittal reformation images, they found cortical disruption in anterior aspect of mid sternal body (white arrow). C. Bone scan after 1 weeks, there was radioactivity in sternal body (white arrow). And there were some activities in lower sacrum due to sacral fractures (black arrowhead).
Reference
-
1. Shanmuganathan K, Mirvis SE. Imaging diagnosis of nonaortic thoracic injury. Radiol Clin North Am. 1999; 37:533–551. vi2. Collins J. Chest wall trauma. J Thorac Imaging. 2000; 15:112–119.3. Recinos G, Inaba K, Dubose J, Barmparas G, Teixeira PG, Talving P, et al. Epidemiology of sternal fractures. Am Surg. 2009; 75:401–404.4. Kaewlai R, Avery LL, Asrani AV, Novelline RA. Multidetector CT of blunt thoracic trauma. Radiographics. 2008; 28:1555–1570.5. Johnson I, Branfoot T. Sternal fracture--a modern review. Arch Emerg Med. 1993; 10:24–28.6. Goodman LR, Teplick SK, Kay H. Computed tomography of the normal sternum. AJR Am J Roentgenol. 1983; 141:219–223.7. Shin MS, Berland LL, Ho KJ. Computed tomography evaluation of primary and secondary sternal neoplasms. J Comput Tomogr. 1986; 10:27–32.8. von Garrel T, Ince A, Junge A, Schnabel M, Bahrs C. The sternal fracture: radiographic analysis of 200 fractures with special reference to concomitant injuries. J Trauma. 2004; 57:837–844.9. Huggett JM, Roszler MH. CT findings of sternal fracture. Injury. 1998; 29:623–626.10. Mirvis SE. Imaging of acute thoracic injury: the advent of MDCT screening. Semin Ultrasound CT MR. 2005; 26:305–331.11. Sangster GP, González-Beicos A, Carbo AI, Heldmann MG, Ibrahim H, Carrascosa P, et al. Blunt traumatic injuries of the lung parenchyma, pleura, thoracic wall, and intrathoracic airways: multidetector computer tomography imaging findings. Emerg Radiol. 2007; 14:297–310.12. Kim EY, Yang HJ, Sung YM, Hwang KH, Kim JH, Kim HS. Sternal fracture in the emergency department: diagnostic value of multidetector CT with sagittal and coronal reconstruction images. Eur J Radiol. 2012; 81:e708–e711.13. Anne MR, Arthur FD. Grant's Atlas of Anatomy. 12th ed. Philadelphia, PA: Lippincott Williams and Wilkins;2009. p. 10.14. John AM, Robert SH, Ron MW. Rosen's Emergency Medicine. 7th ed. Philadelphia, PA: Mosby Elsevier;2010. p. 388–389.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of Three Dimensional Reconstructive Images for Thoracic Trauma Induced Fractures
- Sagittal Fracture of Cervical Spine: Case Report
- Traumatic Sternal Fracture: Incidence, Causes, and CT Features
- Usefulness of Sagittal CT in Orbital Floor Fracture
- Three-dimensional reformation of computed tomography in the nasal bone fractures
