Comparison of Percutaneous Radiologic Gastrostomy by Using Cone Beam CT and Endoscopic Gastrostomy
- Affiliations
-
- 1Department of Radiology, Chonbuk National University Hospital and Medical School, Jeonju, Korea. ymhan@jbnu.ac.kr
- 2Research Institute of Clinical Medicine, Chonbuk National University Hospital and Medical School, Jeonju, Korea.
- 3Institute of Cardiovascular Research, Chonbuk National University Hospital and Medical School, Jeonju, Korea.
- KMID: 1897255
- DOI: http://doi.org/10.3348/jksr.2014.70.1.17
Abstract
- PURPOSE
To compare the effectiveness of percutaneous radiologic gastrostomy (PRG) by using cone beam CT and percutaneous endoscopic gastrostomy (PEG).
MATERIALS AND METHODS
This study retrospectively reviewed 129 patients who underwent PRG (n = 53) and PEG (n = 76) over a 2-years period. The C-arm cone beam CT images were obtained from all PRG patients before the procedure in order to decide the safest accessing routes. The parameters including technical success rates, complication rates and tube migration rates were all analyzed according to statistical methods.
RESULTS
The success rate of tube placement was higher in PRG than in PEG (100% to 93%, p = 0.08). Minor complications occurred in 5 patients of the PRG group (10%; 5/53, 3 wound infection, 2 blood oozing), and occurred in 6 patients of PEG group (7.9%; 6/76, 5 wound infection, 1 esophageal ulcer). Major complications occurred only in 5 patients of PEG group (6.6%; 5/76, 1 panperitonitis, 4 buried bumper syndrome). There were no statistical differences of minor and major complication rates in the two groups (respectively, p = 0.759, p = 0.078). Tube migration rate was lower in PRG than PEG group (7.5% vs. 38.2%, p < 0.005).
CONCLUSION
PRG using cone beam CT is the effective and safe method, the cone beam CT provides the safest accessing route during gastrostomy. Less tube migration occurs in the PRG than in PEG.
MeSH Terms
Figure
-
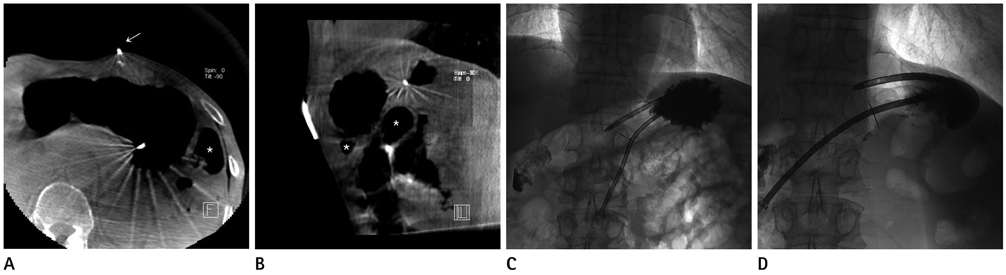
Fig. 1 58-year-old man with dysphagia due to malignant neoplasm of hypopharynx. A. Axial image of cone beam CT was obtained. The metallic marker (arrow) shows appropriate site to puncture. Small bowel (asterisk) is laterally positioned to stomach. B. Sagittal image of cone beam CT shows small bowel loop (asterisk) positioned inferiorly and posteriorly to the stomach. C. Final tubogram shows the gastrostomy catheter is successfully inserted with good position. D. Four month later, gastrostomy tube was changed. The tubogram shows good position and function.

Fig. 2 74-year-old man with dysphagia due to esophageal cancer referred to PRG after failure of PEG procedure. A. PEG was failed due to circumferential luminal narrowing (arrows); pediatric endoscopy with the smallest diameter could not advance more. B. The stomach was distended with air insufflation through the Headhunter catheter (arrows) via nasogastric route. C. The appropriate site was punctured with the needle. The guide wire was inserted through the needle (arrowheads). D. The catheter was inserted through the guide wire. Injection of water-soluble contrast material through the catheter shows the confirmation of good position of catheter tip. Note.-PEG = percutaneous endoscopic gastrostomy, PRG = percutaneous radiologic gastrostomy
Reference
-
1. Saini S, Mueller PR, Gaa J, Briggs SE, Hahn PF, Forman BH, et al. Percutaneous gastrostomy with gastropexy: experience in 125 patients. AJR Am J Roentgenol. 1990; 154:1003–1006.2. O'Keeffe F, Carrasco CH, Charnsangavej C, Richli WR, Wallace S, Freedman RS. Percutaneous drainage and feeding gastrostomies in 100 patients. Radiology. 1989; 172:341–343.3. Halkier BK, Ho CS, Yee AC. Percutaneous feeding gastrostomy with the Seldinger technique: review of 252 patients. Radiology. 1989; 171:359–362.4. van Sonnenberg E, Wittich GR, Cabrera OA, Quinn SF, Casola G, Lee AA, et al. Percutaneous gastrostomy and gastroenterostomy: 2. Clinical experience. AJR Am J Roentgenol. 1986; 146:581–586.5. Walker LG Jr. L. L. Staton, M.D., and the first successful gastrostomy in America. Surg Gynecol Obstet. 1984; 158:387–388.6. Gauderer MW, Ponsky JL, Izant RJ Jr. Gastrostomy without laparotomy: a percutaneous endoscopic technique. J Pediatr Surg. 1980; 15:872–875.7. Preshaw RM. A percutaneous method for inserting a feeding gastrostomy tube. Surg Gynecol Obstet. 1981; 152:658–660.8. Given MF, Hanson JJ, Lee MJ. Interventional radiology techniques for provision of enteral feeding. Cardiovasc Intervent Radiol. 2005; 28:692–703.9. Blondet A, Lebigot J, Nicolas G, Person B, Laccoureye L, Goura E, et al. [Image-guided percutaneous gastrostomy]. J Radiol. 2008; 89(9 Pt 1):1065–1075.10. Levin DC, Matteucci T. "Turf battles" over imaging and interventional procedures in community hospitals: survey results. Radiology. 1990; 176:321–324.11. Sanchez RB, vanSonnenberg E, D'Agostino HB, Goodacre BW, Moyers P, Casola G. CT guidance for percutaneous gastrostomy and gastroenterostomy. Radiology. 1992; 184:201–205.12. Teichgräber UK, Streitparth F, Cho CH, Gebauer B, Ricke J, Benter T. Percutaneous push-through gastrostomy by applying a CT-guided gastropexy. J Vasc Interv Radiol. 2011; 22:1149–1152.13. de Bucourt M, Collettini F, Althoff C, Streitparth F, Greupner J, Hamm B, et al. CT fluoroscopy-guided percutaneous gastrostomy with loop gastropexy and peel-away sheath trocar technique in 31 amyotrophic lateral sclerosis patients. Acta Radiol. 2012; 53:285–291.14. Cardella JF, Kundu S, Miller DL, Millward SF, Sacks D. Society of Interventional Radiology. Society of Interventional Radiology clinical practice guidelines. J Vasc Interv Radiol. 2009; 20:7 Suppl. S189–S191.15. Wollman B, D'Agostino HB, Walus-Wigle JR, Easter DW, Beale A. Radiologic, endoscopic, and surgical gastrostomy: an institutional evaluation and meta-analysis of the literature. Radiology. 1995; 197:699–704.16. Hoffer EK, Cosgrove JM, Levin DQ, Herskowitz MM, Sclafani SJ. Radiologic gastrojejunostomy and percutaneous endoscopic gastrostomy: a prospective, randomized comparison. J Vasc Interv Radiol. 1999; 10:413–420.17. Wollman B, D'Agostino HB. Percutaneous radiologic and endoscopic gastrostomy: a 3-year institutional analysis of procedure performance. AJR Am J Roentgenol. 1997; 169:1551–1553.18. Blondet A, Lebigot J, Nicolas G, Boursier J, Person B, Laccoureye L, et al. Radiologic versus endoscopic placement of percutaneous gastrostomy in amyotrophic lateral sclerosis: multivariate analysis of tolerance, efficacy, and survival. J Vasc Interv Radiol. 2010; 21:527–533.19. Nicholson FB, Korman MG, Richardson MA. Percutaneous endoscopic gastrostomy: a review of indications, complications and outcome. J Gastroenterol Hepatol. 2000; 15:21–25.20. Schrag SP, Sharma R, Jaik NP, Seamon MJ, Lukaszczyk JJ, Martin ND, et al. Complications related to percutaneous endoscopic gastrostomy (PEG) tubes. A comprehensive clinical review. J Gastrointestin Liver Dis. 2007; 16:407–418.21. Itkin M, DeLegge MH, Fang JC, McClave SA, Kundu S, Janne d'Othee B, et al. Multidisciplinary practical guidelines for gastrointestinal access for enteral nutrition and decompression from the Society of Interventional Radiology and American Gastroenterological Association (AGA) Institute, with endorsement by Canadian Interventional Radiological Association (CIRA) and Cardiovascular and Interventional Radiological Society of Europe (CIRSE). J Vasc Interv Radiol. 2011; 22:1089–1106.22. Löser C, Aschl G, Hébuterne X, Mathus-Vliegen EM, Muscaritoli M, Niv Y, et al. ESPEN guidelines on artificial enteral nutrition--percutaneous endoscopic gastrostomy (PEG). Clin Nutr. 2005; 24:848–861.23. Orth RC, Wallace MJ, Kuo MD. Technology Assessment Committee of the Society of Interventional Radiology. C-arm cone-beam CT: general principles and technical considerations for use in interventional radiology. J Vasc Interv Radiol. 2008; 19:814–820.24. Kim SM, Kim SM, Yang SW, Lee TH, Im EH, Choi YW, et al. Two cases of buried bumper syndrome after percutaneous endoscopic gastrostomy. Korean J Med. 2009; 76:722–726.25. Ryan JM, Hahn PF, Boland GW, McDowell RK, Saini S, Mueller PR. Percutaneous gastrostomy with T-fastener gastropexy: results of 316 consecutive procedures. Radiology. 1997; 203:496–500.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Updates on Percutaneous Radiologic Gastrostomy/Gastrojejunostomy and Jejunostomy
- Percutaneous Radiologic Gastrostomy in a Locked-in Syndrome Patient : A case report
- Percutaneous Endoscopic Gastrostomy Through the Sinus Tract of a Surgical Gastrostomy
- Long Term Efficacy of Percutaneous Endoscopic Gastrostomy
- A Case of Buried Bumper Syndrome; A case report
