Treatment of Anchor Suture with Kirschner Wires Fixation for Chronic Perilunate Dislocation
- Affiliations
-
- 1Department of Orthopedic Surgery, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. kiga9@hallym.or.kr
- KMID: 1896910
- DOI: http://doi.org/10.12790/jkssh.2014.19.4.200
Abstract
- Chronic lunate dislocations are very rare injuries comprising of less than 10% of all wrist injuries. Volar lunate dislocations account for less than 3% of perilunate dislocations. We present a case of a missed volar lunate dislocation for 6months after initial injury. He fell down and had hyperextension injury during his sports activity. When the patient visit in our hospital, neurologic symptom was developed in distribution of median nerve. Tingling sensation and radiation symptom was found in affected hand. A plain radiograph revealed a volar lunate dislocation. Nerve conduction studies confirmed compression of the median nerve at the wrist, carpal tunnel level. Operation was performed with open reduction of lunate, fixation with K-wires and anchor suture. The outcome was excellent in relieving pain, function, range of motion, grip strength. There was improvement in Mayo wrist score and disabilities of the arm, shoulder and hand score. So we report a patient and a operation technique which can be considered in similar cases.
Keyword
MeSH Terms
Figure
-

Fig. 1. (A) Anteroposterior view. (B) Lateral radiographs of the wrist before reduction and fixation. (C) Scapholunate angle (S-L), 13.6°.
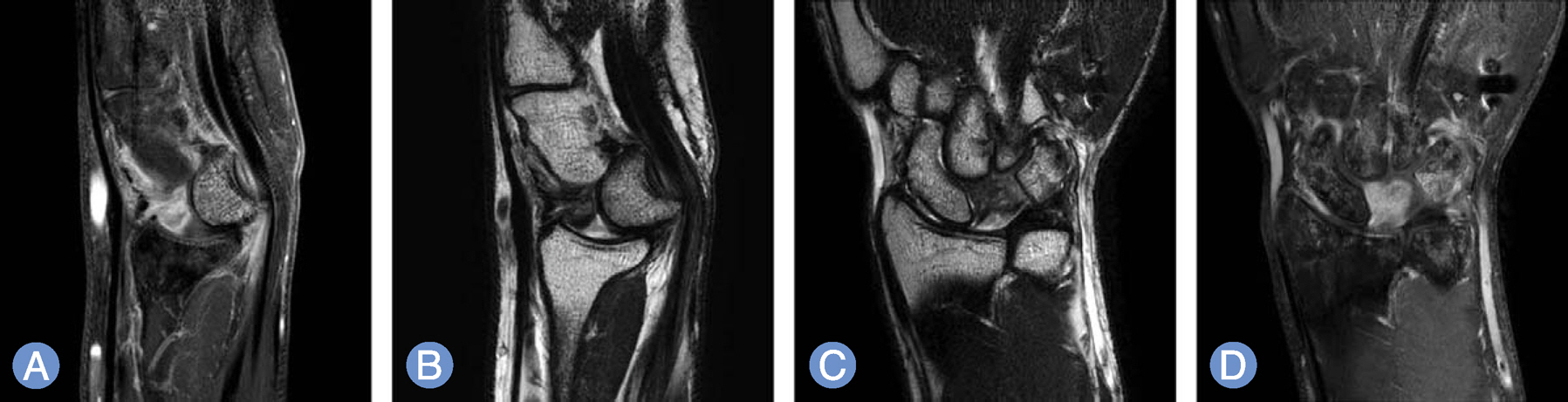
Fig. 2. (A) Magnetic resonance image sagittal view before operation (T2). (B) T1 enhance. (C) Coronal view before operation (T2). (D) T1 enhance.

Fig. 3. Intraoperative finding. (A) Pre-reduction. (B) Post-reduction. (C) Intraoperative X-ray finding with anchor suture and K-wire fixation.

Fig. 4. Schematic image of location for anchor suture.

Fig. 5. (A) Anteroposterior view. (B) Lateral radiographs of the wrist following open reduction and fixation. (C) Scapholunate angle: 50.2°.

Fig. 6. (A) Anteroposterior view. (B) Lateral radiographs of the wrist following 12 months after surgery. (C) Scapholunate angle: 51.4°.
Reference
-
1. Sauder DJ, Athwal GS, Faber KJ, Roth JH. Perilunate injuries. Orthop Clin North Am. 2007; 38:279–88.
Article2. Chung MS, Suk SI, Lee CS. Clinical study of the trans-scaphoid perilunar dislocation. J Korean Fracture Soc. 1988; 1:43–53.
Article3. Green DP, O'Brien ET. Open reduction of carpal dislocations: indications and operative techniques. J Hand Surg Am. 1978; 3:250–65.
Article4. Herzberg G. Acute dorsal trans-scaphoid perilunate dislocations: open reduction and internal fixation. Tech Hand Up Extrem Surg. 2000; 4:2–13.5. Park JW, Lee KS, Kim SK, et al. Operative treatment of perilunar fracture dislocation. J Korean Soc Surg Hand. 2002; 7:23–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Surgical Treatment of Type V Acute Acromioclavicular Joint Dislocation Using Suture Anchor and Kirschner Wire
- Perilunate Dislocation and Perilunate Fracture-Dislocation
- Surgical Treatment Using Anchor Suture of Coracoid Process Fracture with Acromioclavicular Joint Dislocation: A Case Report
- Carpometacarpal Joint Dislocation of the Thumb Associated with Fracture of the Trapezium: A Case Report
- A Case of Dislocation of the Hamte Bone
