Upper terminal of the inferior vena cava and development of the heart atriums: a study using human embryos
- Affiliations
-
- 1Department of Anatomy, Chonbuk National University Medical School, Jeonju, Korea. 407kk@hanmail.net
- 2Department of Surgery, Daejeon Sun Hospital, Daejeon, Korea.
- 3Institute of Embryology, Universidad Complutense, Madrid, Spain.
- 4Division of Internal Medicine, Iwamizawa Asuka Hospital, Iwamizawa, Japan.
- 5Department of Surgery and Biomedical Research Institute, Chonbuk National University Hospital, Jeonju, Korea.
- KMID: 1882602
- DOI: http://doi.org/10.5115/acb.2014.47.4.236
Abstract
- In the embryonic heart, the primitive atrium is considered to receive the bilateral sinus horns including the upper terminal of the inferior vena cava (IVC). To reveal topographical anatomy of the embryonic venous pole of the heart, we examined horizontal serial paraffin sections of 15 human embryos with crown-rump length 9-31 mm, corresponding to a gestational age of 6-7 weeks or Carnegie stage 14-16. The IVC was often fixed to the developing right pulmonary vein by a mesentery-like fibrous tissue. Rather than the terminal portion of the future superior vena cava, the IVC contributed to form a right-sided atrial lumen at the stage. The sinus venosus or its left horn communicated with the IVC in earlier specimens, but in later specimens, the left atrium extended caudally to separate the sinus and IVC. In contrast, the right atrium consistently extended far caudally, even below the sinus horn, along the IVC. A small (or large) attachment between the left (or right) atrium and IVC in adult hearts seemed to be derived from the left (or right) sinus valve. This hypothesis did not contradict with the incorporation theory of the sinus valves into the atrial wall. Variations in topographical anatomy around the IVC, especially of the sinus valves, might not always depend on the stages but partly in individual differences.
Keyword
MeSH Terms
Figure
-
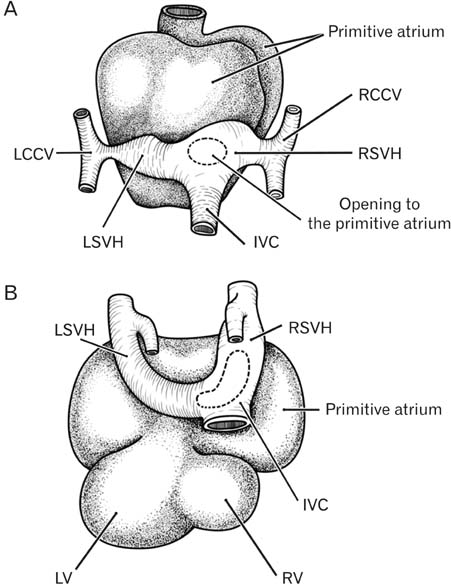
Fig. 1 Schematic representations of the early fetal atrium and venous routes. Dorsal views. In panels (A) and (B), a structure large as the ventricles (LV, left ventricle; RV, right ventricle), termed the primitive atrium, is evident in the ventral side of the sinus venosus horns (left sinus venosus horn [LVSH], right sinus venosus horn [RVSH]) and inferior vena cava (IVC). LCCV, left common cardinal vein; RCCV, right common cardinal vein.
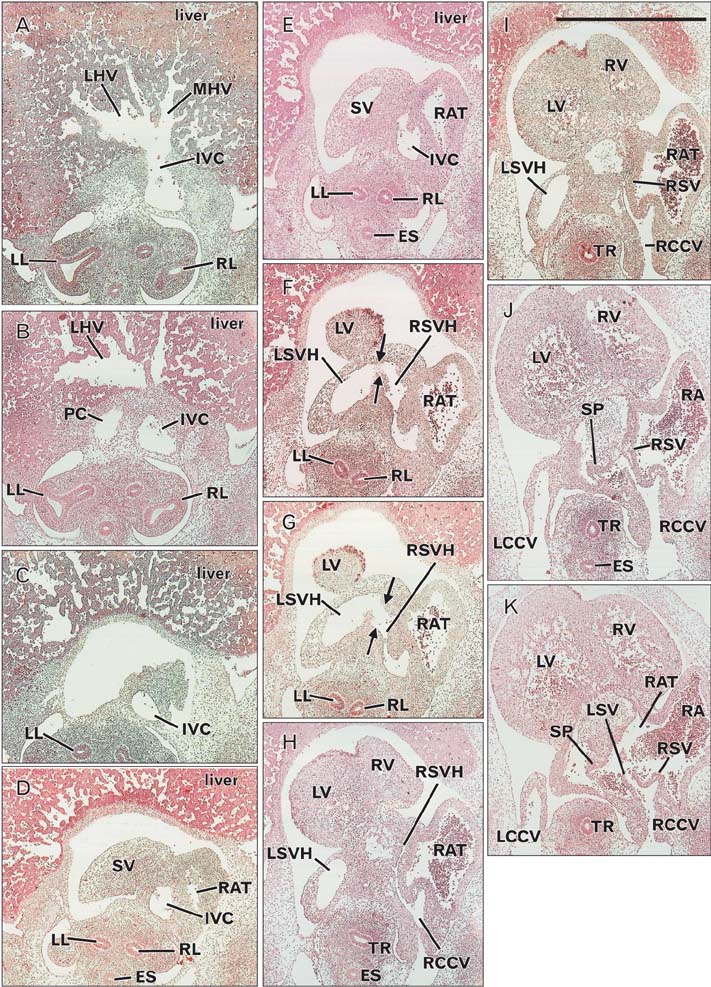
Fig. 2 Inferior vena cava terminal in an embryo of crown-rump length 10 mm. Panels A and K show the most caudal and cranial sides of the figure, respectively. The intervals between panels were 0.05 mm (A, B), 0.16 mm (B, C), 0.1 mm (C, D), 0.06 mm (D, E), 0.02 mm (E, F), 0.01 mm (F, G), 0.14 mm (G, H), 0.06 mm (H, I), 0.16 mm (I, J), and 0.1 mm ( J, K). A part of the sinus venosus (SV) was observed on the left side of the inferior vena cava (IVC) (D, E), communicating with the left horn (LSVH) (arrows in panels F and G). The left sinus horn extended cranially (H, I), continuing to the left common cardinal vein (LCCV) ( J). The right sinus venosus horn (RSVH) opened to the right atrium (RAT) (K) 0.35 mm to the cranial side of the opening of the right common cardinal vein (RCCV) or superior vena cava (H). ES, esophagus; LHV, left hepatic vein; LL, left lung ; LSV, left sinus valve; LSVH, left sinus venosus horn; LV, left ventricle; MHV, middle hepatic vein; PC, pericardium; RA, right auricle; RL, right lung; RSV, right sinus valve; RV, right ventricle; SP, septum primum; TR, trachea. All panels were prepared at the same magnification. Scale bar=1 mm.
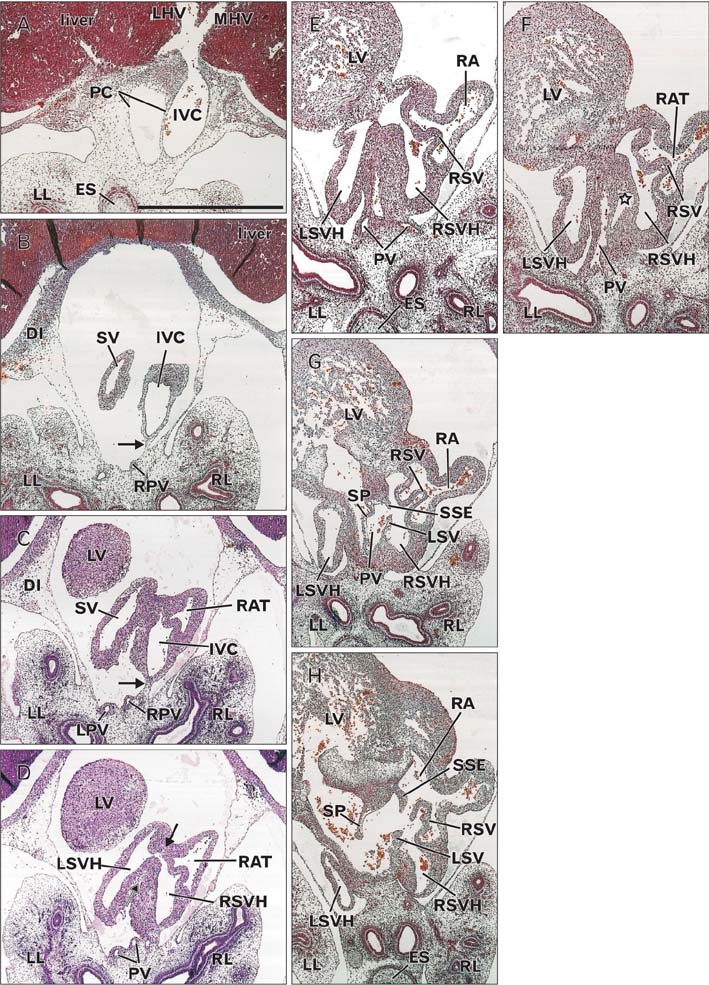
Fig. 3 Inferior vena cava terminal in an embryo of crown-rump length 16.5 mm. Panels (A) and (G) show the most caudal and cranial sides of the figure, respectively. The intervals between panels were 0.5 mm (A, B), 0.05 mm (B, C), 0.15 mm (C, D), 0.05 mm (D, E), 0.1 mm (E, F), and 0.8 mm (F, G). A part of the sinus venosus (SV) was present on the left side of the inferior vena cava (IVC) (D, E) and communicated with the coronary sinus (CS) (F). The right atrium (RAT) was attached to the ventral aspect of the IVC (D, E). Communication between the right sinus venosus horn (RSVH) and the right atrium (G) was located in 0.6 mm caudal side of the right common cardinal venous opening (not shown). The arrow in panel (F) indicates a fibrous connection between the right pulmonar y ve in (RPV ) and the IVC. AO, aorta; DI, diaphragm; ES, esophagus; LAT, left atrium; LHV, left hepatic vein; LL, left lung; LPV, left pulmonary vein; LSV, left sinus valve; LV, left ventricle; MHV, middle hepatic vein; PC, pericardium; RA, right auricle; RAT, right atrium; RL, right lung; RSV, right sinus valve; RV, right ventricle; SP, septum primum; SSE, septum secundum; SV, sinus venosum. All panels were prepared at the same magnification. Scale bar=1 mm.
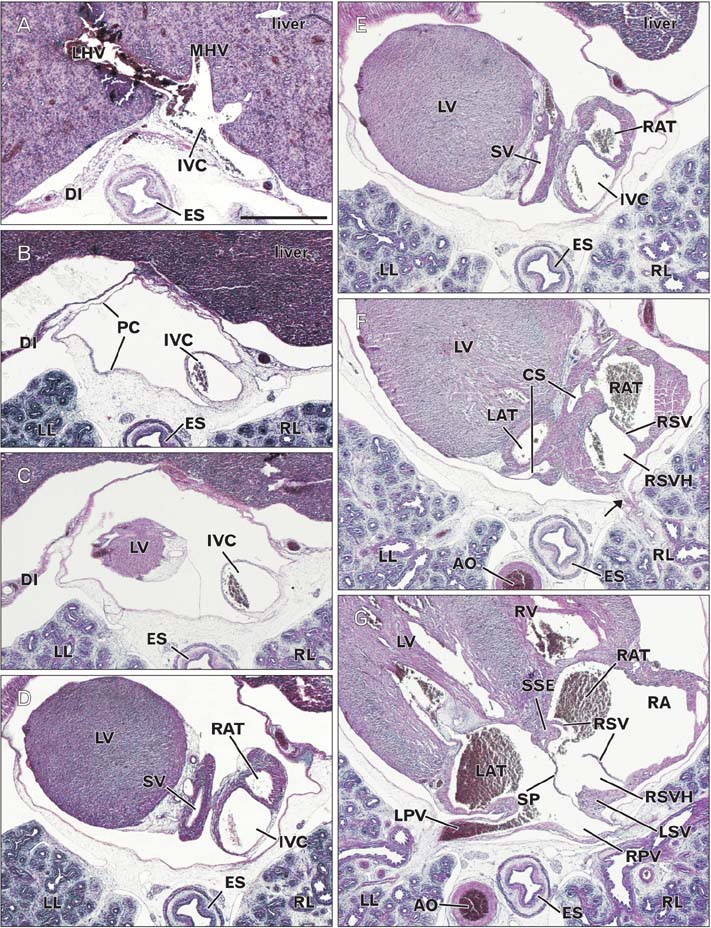
Fig. 4 Inferior vena cava terminal in an embryo of crown-rump length 16.5 mm. Panels (A) and (G) show the most caudal and cranial sides of the figure, respectively. The intervals between panels were 0.5 mm (A, B), 0.05 mm (B, C), 0.15 mm (C, D), 0.05 mm (D, E), 0.1 mm (E, F), and 0.8 mm (F, G). A part of the sinus venosus (SV) was present on the left side of the inferior vena cava (IVC) (D, E) and communicated with the coronary sinus (CS) (F). The right atrium (RAT) was attached to the ventral aspect of the IVC (D, E). Communication between the right sinus venosus horn (RSVH) and the right atrium (G) was located in 0.6 mm caudal side of the right common cardinal venous opening (not shown). The arrow in panel (F) indicates a fibrous connection between the right pulmonar y ve in (RPV ) and the IVC. AO, aorta; DI, diaphragm; ES, esophagus; LAT, left atrium; LHV, left hepatic vein; LL, left lung; LPV, left pulmonary vein; LSV, left sinus valve; LV, left ventricle; MHV, middle hepatic vein; PC, pericardium; RA, right auricle; RAT, right atrium; RL, right lung; RSV, right sinus valve; RV, right ventricle; SP, septum primum; SSE, septum secundum; SV, sinus venosum. All panels were prepared at the same magnification. Scale bar=1 mm.
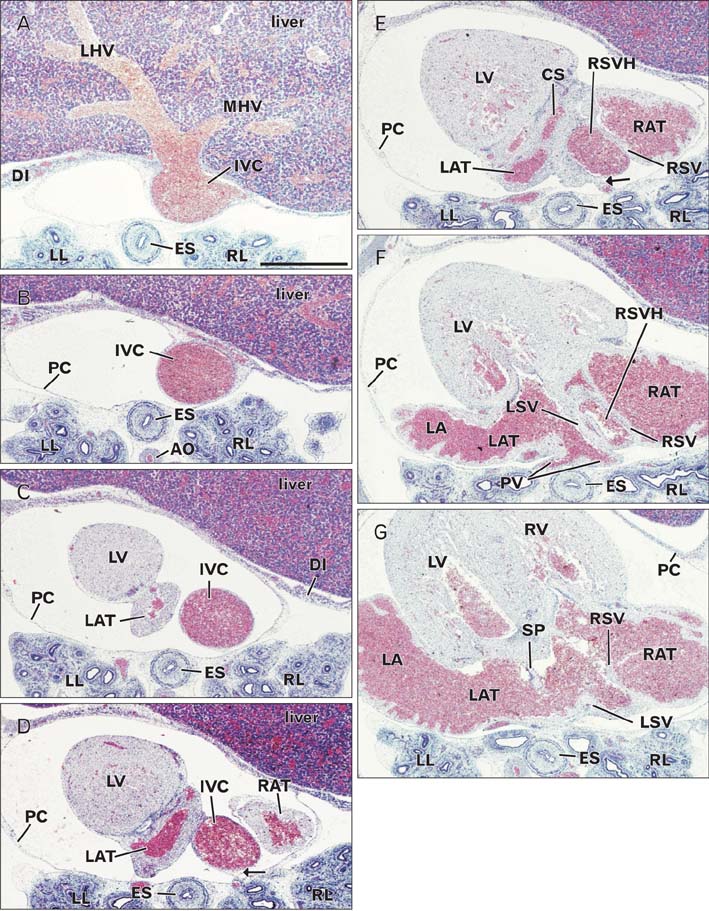
Fig. 5 Inferior vena cava terminal in an embryo of crown-rump length 21 mm. Panels (A) and (G) show the most caudal and cranial sides of the figure, respectively. Intervals between panels were 0.2 mm (A, B), 0.3 mm (B, C), 0.2 mm (C, D), 0.1 mm (D, E), 0.2 mm (E, F), and 0.4 mm (F, G). The left atrium (LAT) was present on the left side of the inferior vena cava (IVC) (C, D). No left sinus horn was visible. The right atrium (RAT) was attached to the ventral aspect of the right sinus venosus horn (RSVH) (E, F), which opened to the RAT and LAT (G) 0.7 mm to the caudal side of the opening of the right common cardinal vein (not shown). The arrows in panels (D) and (E) indicate a fibrous connection between the right pulmonary vein and the IVC and RSVH. AO, aorta; CS, coronary sinus; DI, diaphragm; ES, esophagus; LA, left auricle; LHV, left hepatic vein; LL, left lung; LSV, left sinus valve; LV, left ventricle; MHV, middle hepatic vein; PC, pericardium; PV, pulmonary veins; RL, right lung; RSV, right sinus valve; RV, right ventricle; SP, septum primum. All panels were prepared at the same magnification. Scale bar=1 mm.

Fig. 6 Inferior vena cava terminal in an embryo of crown-rump length 22 mm. Panels (A) and (H) show the most caudal and cranial sides of the figure, respectively. The intervals between panels were 0.1 mm (A, B), 0.05 mm (B, C), 0.15 mm (C, D), 0.05 mm (D, E), 0.1 mm (E, F), and 0.8 mm (F, G), respectively. A part of the sinus venosus was present on the left side of the inferior vena cava (IVC) (D, E) and communicated with the coronary sinus (CS) (F). The right atrium (RAT) was attached to the ventral aspect of the IVC (D, E) and communicated with the right sinus venosus horn (RSVH) (H) 0.6 mm to the caudal side of the opening of the right common cardinal vein (not shown). The arrow in panel (F) indicates a fibrous connection between the right pulmonary vein (RPV) and the IVC. CS, coronary sinus; ES, esophagus; GCV, great cardiac vein; LA, left auricle; LAT, left atrium; LL, left lung ; LPV, left pulmonary vein; LSV, left sinus valve; LSVH, left sinus venosus horn; LV, left ventricle; PV, pulmonary veins; RA, right auricle; RL, right lung; RSV, right sinus valve; RV, right ventricle; SSE, septum secundum. All panels were prepared at the same magnification. Scale bar=1 mm.

Fig. 7 Topographical anatomy of the early inferior vena cava and its surroundings. Dorsal views of embryos with 9-31 mm crown-rump length. Panel (A) displays the initial morphology in which the left atrium has not yet developed, while panel (B) exhibits the developing phase of the left-sided structures. Instead of the primitive atrium (a common chamber), the right atrium (RAT) was as large as the left sinus venosus horn and extend caudally along the inferior vena cava (IVC). Opening of the sinus venosus to the atrium (Fig. 1) corresponds to the upper end of the IVC (or the right sinus venosus horn) that is sandwiched by the left and right sinus valves (LSV, RSV). The developing pulmonary vein (PV) is connected with the dorsal aspect of the IVC by a fibrous structure (star). LAT, left atrium; LCCV, left common cardinal vein; LSVH, left sinus venosus horn; LV, left ventricle; RCCV, right common cardinal vein; RSVH, right sinus venosus horn; RV, right ventricle.
Reference
-
1. Anderson RH, Brown NA, Moorman AF. Development and structures of the venous pole of the heart. Dev Dyn. 2006; 235:2–9.2. Sizarov A, Anderson RH, Christoffels VM, Moorman AF. Three-dimensional and molecular analysis of the venous pole of the developing human heart. Circulation. 2010; 122:798–807.3. Dickson AD. The development of the ductus venosus in man and the goat. J Anat. 1957; 91:358–368.4. Mavrides E, Moscoso G, Carvalho JS, Campbell S, Thilaganathan B. The anatomy of the umbilical, portal and hepatic venous systems in the human fetus at 14-19 weeks of gestation. Ultrasound Obstet Gynecol. 2001; 18:598–604.5. Collardeau-Frachon S, Scoazec JY. Vascular development and differentiation during human liver organogenesis. Anat Rec (Hoboken). 2008; 291:614–627.6. Blom NA, Gittenberger-de Groot AC, Jongeneel TH, DeRuiter MC, Poelmann RE, Ottenkamp J. Normal development of the pulmonary veins in human embryos and formulation of a morphogenetic concept for sinus venosus defects. Am J Cardiol. 2001; 87:305–309.7. Steding G, Xu JW, Seidl W, Männer J, Xia H. Developmental aspects of the sinus valves and the sinus venosus septum of the right atrium in human embryos. Anat Embryol (Berl). 1990; 181:469–475.8. Webb S, Kanani M, Anderson RH, Richardson MK, Brown NA. Development of the human pulmonary vein and its incorporation in the morphologically left atrium. Cardiol Young. 2001; 11:632–642.9. Hayashi S, Fukuzawa Y, Rodríguez-Vázquez JF, Cho BH, Verdugo-López S, Murakami G, Nakano T. Pleuroperitoneal canal closure and the fetal adrenal gland. Anat Rec (Hoboken). 2011; 294:633–644.10. Rodríguez-Vázquez JF, Kim JH, Verdugo-López S, Murakami G, Cho KH, Asakawa S, Abe S. Human fetal hyoid body origin revisited. J Anat. 2011; 219:143–149.11. Miyake N, Hayashi S, Kawase T, Cho BH, Murakami G, Fujimiya M, Kitano H. Fetal anatomy of the human carotid sheath and structures in and around it. Anat Rec (Hoboken). 2010; 293:438–445.12. Bartram U, Van Praagh S, Keane JF, Lang P, van der Velde ME, Van Praagh R. Mitral and aortic atresia associated with hypoplastic right lung, crossover segment of right lower lobe, and anomalous scimitar-like right pulmonary venous connection with inferior vena cava: clinical, angiocardiographic, and autopsy findings in a rare case. Pediatr Dev Pathol. 1998; 1:413–419.13. Sadler TW. Langman's medical embryology. 7th ed. Baltimore: Williams & Wilkins;1995.14. Moore KL, Persaud TV. The developing human: clinically oriented embryology. 6th ed. Philadelphia: W. B. Saunders;1998.
