The Clinical Characteristics of Subependymal Giant Cell Astrocytoma: Five Cases
- Affiliations
-
- 1Department of Neurosurgery, Chonnam National University Research Institute of Medical Sciences, Chonnam National University Hwasun Hospital & Medical School, Hwasun, Korea. jung-ty@chonnam.ac.kr
- 2Department of Pediatrics, Chonnam National University Research Institute of Medical Sciences, Chonnam National University Hwasun Hospital & Medical School, Hwasun, Korea.
- 3Department of Pathology, Chonnam National University Research Institute of Medical Sciences, Chonnam National University Hwasun Hospital & Medical School, Hwasun, Korea.
- KMID: 1882010
- DOI: http://doi.org/10.14791/btrt.2015.3.1.44
Abstract
- In this study, we reviewed the clinical characteristics of five cases of subependymal giant cell astrocytoma (SEGA) at our hospital between May 1997 and July 2012. The median age was 18 years old (range, 8 to 26). The clinical symptoms were presented as seizure in two patients and headache in three patients. All the tumors were located near the foramen of Monro. The median size of the tumors was 2.5 cm (range, 1.9-4.0). Two patients showed the solitary lesion, and three had subependymal nodules and cortical tubers. The median follow-up duration was 7.4 years (range, 2.0-14.3). Three patients were associated with the tuberous sclerosis complex (TSC). Four patients showed the SEGA at the first presentation and one patient experienced the 1.9 cm-sized growing mass during 7.7 years follow-up after the diagnosis of the TSC. The mass was totally removed in four patients and subtotally in one. Postoperatively, one patient took the medication for the seizure, which was controllable. The subtotally removed mass showed the recurrence postoperative 4.1 years later, and the recurred mass was stable for 4.5 years after the recurrence. The clinical follow-up study of the SEGA showed an indolent behavior before and after the surgery.
MeSH Terms
Figure
-
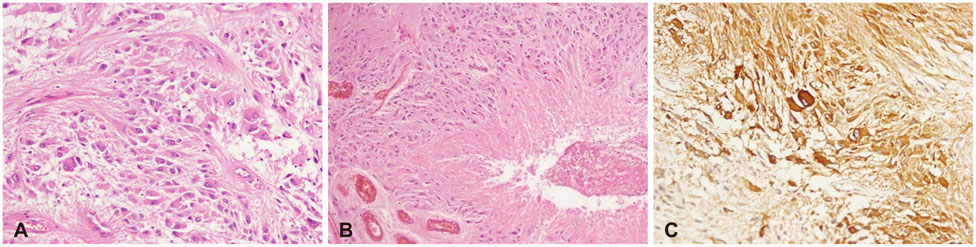
Fig. 1 Pathological findings of subependymal giant cell astrocytoma. A: Pathology shows the pleomorphic multinucleated eosinophilic tumor cells with abundant cytoplasm and these elongated tumor cells formed streams (hematoxylin and eosin staining, original magnification ×200). B: The tumor cells with abundant cytoplasm are clustered and arranged in perivascular pseudopalisading pattern (hematoxylin and eosin staining, original magnification ×100). C: The tumor cells are immune-positive for microtubule-associated protein 2 (original magnification ×200).
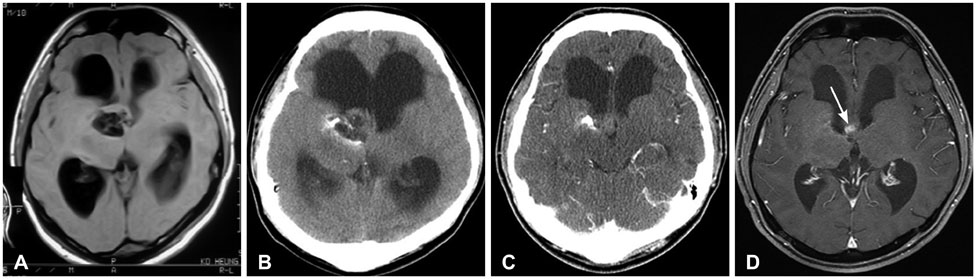
Fig. 2 Radiological findings of case 2. A: Brain MRI shows 3 cm-sized solitary lesion near to the foramen of Monro with iso-signal intensity on T1-weighted images. B: Brain CT reveals that the mass was associated with cyst and calcification. C: The mass is subtotally removed, because of the adhesion of the hypothalamus. D: The follow-up MRI shows a 0.8 cm nodular enhancing lesion (arrow) in the right side of the septum pellucidum.
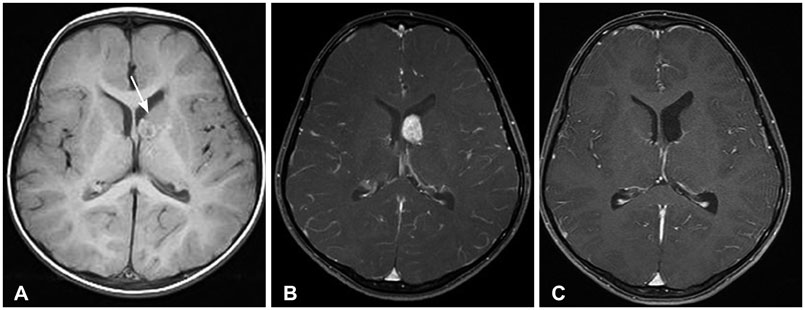
Fig. 3 Radiological findings of case 4. A: Brain MRI shows the 1 cm-sized mass (arrow) adjacent to the foramen of Monro with iso-signal intensity on T1-weighted images. B: Brain MRI displays 1.9 cm-sized enlarged lesion with contrast enhancement. C: There was no recurred lesion for two years after the operation.
Cited by 1 articles
-
Subependymal Giant Cell Astrocytoma Presenting with Tumoral Bleeding: A Case Report
Jae-Young Kim, Tae-Young Jung, Kyung-Hwa Lee, Seul-Kee Kim
Brain Tumor Res Treat. 2017;5(1):37-41. doi: 10.14791/btrt.2017.5.1.37.
Reference
-
1. Roth J, Roach ES, Bartels U, et al. Subependymal giant cell astrocytoma: diagnosis, screening, and treatment. Recommendations from the International Tuberous Sclerosis Complex Consensus Conference 2012. Pediatr Neurol. 2013; 49:439–444.
Article2. Crino PB, Nathanson KL, Henske EP. The tuberous sclerosis complex. N Engl J Med. 2006; 355:1345–1356.
Article3. Northrup H, Krueger DA. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 Iinternational Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013; 49:243–254.4. Adriaensen ME, Schaefer-Prokop CM, Stijnen T, Duyndam DA, Zonnenberg BA, Prokop M. Prevalence of subependymal giant cell tumors in patients with tuberous sclerosis and a review of the literature. Eur J Neurol. 2009; 16:691–696.
Article5. Shepherd CW, Scheithauer BW, Gomez MR, Altermatt HJ, Katzmann JA. Subependymal giant cell astrocytoma: a clinical, pathological, and flow cytometric study. Neurosurgery. 1991; 28:864–868.
Article6. Katz JS, Milla SS, Wiggins GC, Devinsky O, Weiner HL, Roth J. Intraventricular lesions in tuberous sclerosis complex: a possible association with the caudate nucleus. J Neurosurg Pediatr. 2012; 9:406–413.
Article7. Shepherd CW, Gomez MR, Lie JT, Crowson CS. Causes of death in patients with tuberous sclerosis. Mayo Clin Proc. 1991; 66:792–796.
Article8. Chow CW, Klug GL, Lewis EA. Subependymal giant-cell astrocytoma in children. An unusual discrepancy between histological and clinical features. J Neurosurg. 1988; 68:880–883.9. Telfeian AE, Judkins A, Younkin D, Pollock AN, Crino P. Subependymal giant cell astrocytoma with cranial and spinal metastases in a patient with tuberous sclerosis. Case report. J Neurosurg. 2004; 100:5 Suppl Pediatrics. 498–500.10. Sterman H, Furlan AB, Matushita H, Teixeira MJ. Subependymal giant cell astrocytoma associated with tuberous sclerosis presenting with intratumoral bleeding. Case report and review of literature. Childs Nerv Syst. 2013; 29:335–339.
Article11. de Ribaupierre S, Dorfmüller G, Bulteau C, et al. Subependymal giant-cell astrocytomas in pediatric tuberous sclerosis disease: when should we operate? Neurosurgery. 2007; 60:83–89. discussion 89-90.12. Matsumura H, Takimoto H, Shimada N, Hirata M, Ohnishi T, Hayakawa T. Glioblastoma following radiotherapy in a patient with tuberous sclerosis. Neurol Med Chir (Tokyo). 1998; 38:287–291.
Article13. Krueger DA, Care MM, Holland K, et al. Everolimus for subependymal giant-cell astrocytomas in tuberous sclerosis. N Engl J Med. 2010; 363:1801–1811.
Article14. Franz DN, Belousova E, Sparagana S, et al. Efficacy and safety of everolimus for subependymal giant cell astrocytomas associated with tuberous sclerosis complex (EXIST-1): a multicentre, randomised, placebo-controlled phase 3 trial. Lancet. 2013; 381:125–132.
Article15. Franz DN, Leonard J, Tudor C, et al. Rapamycin causes regression of astrocytomas in tuberous sclerosis complex. Ann Neurol. 2006; 59:490–498.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of tuberous sclerosis developing with subependymal giant-cell astrocytoma
- A Case of Subependymal Giant Cell Astrocytoma in the Absence of Tuberous Sclerosis: Case Report
- A Case of Tuberous Sclerosis Complex Developing with Subependymal Giant-Cell Astrocytoma and Hydrocephalus
- Subependymal Giant Cell Astrocytoma with a Large Third Ventricular Hematoma
- A Case of Subependymal Giant Cell Astrocytoma associated with Tuberous Sclerosis(Case Report)
