Updates on Treatment of Femoral Head Fractures
- Affiliations
-
- 1Department of Orthopaedic Surgery, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. bakpaker@hanmail.net
- KMID: 1851951
- DOI: http://doi.org/10.4055/jkoa.2015.50.3.171
Abstract
- Fracture of the femoral head is relatively uncommon and usually caused by high energy injury. The femoral head fracture combined with hip dislocation results in severe damage to the hip joint, and therefore has been associated with poor functional outcome. The principle of the treatment is composed of urgent reduction of the dislocated hip and early anatomical reduction, with the goal of restoring a congruent and stable hip. In an effort to reach that goal, several methods have been used for treatment of the fracture after closed reduction of the hip. The purpose of this article is to review the indication of surgery, surgical methods, surgical approach, and clinical outcomes.
Keyword
MeSH Terms
Figure
-
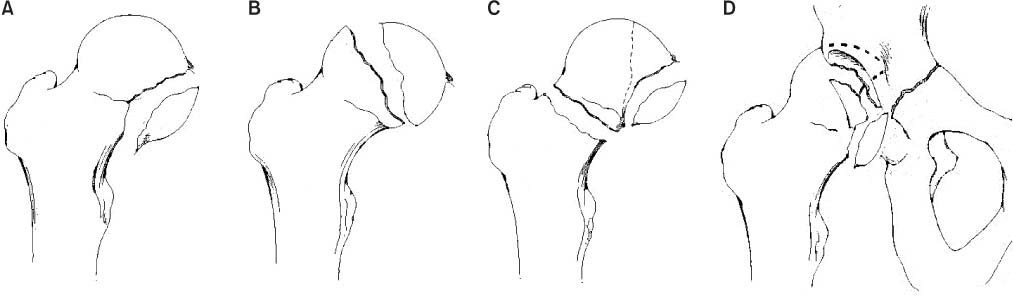
Figure 1 The Pipkin classification. (A) Type I, femoral head fracture inferior to the fovea centralis. (B) Type II, fracture extended superior to the fovea centralis. (C) Type III, any femoral head fracture with an associated femoral neck fracture. (D) Type IV, any femoral head fracture with an associated acetabular fracture.
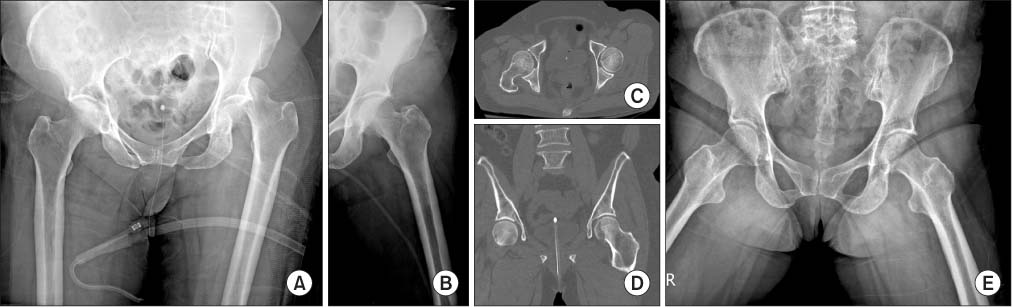
Figure 2 (A) A 68-year-old female had a left hip dislocation with Pipkin type I femoral head fracture. (B) Anteroposterior of both hips and (C, D) computed tomography showing congruent hip and anatomical reduction (<2 mm) after closed reduction. (E) One-year-follow up X-ray showing no evidence of osteonecrosis of the femoral head or arthritis.
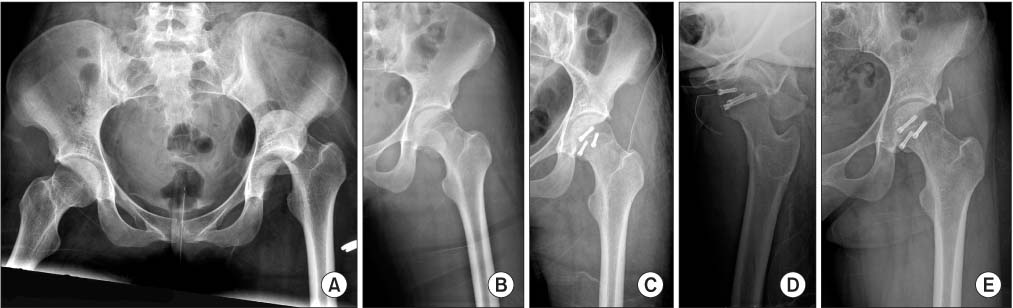
Figure 3 (A) A 24-year-old female had a left hip dislocation with Pipkin type II femoral head fracture. (B) Anteroposterior of both hips showing successful reduction, but non-anatomical reduction of the femoral head. (C, D) Internal fixation was performed with headless screws using the Smith-Peterson approach. (E) Two-year-follow up X-ray demonstrating heterotopic ossification, but no evidence of osteonecrosis of the femoral head or arthritis.
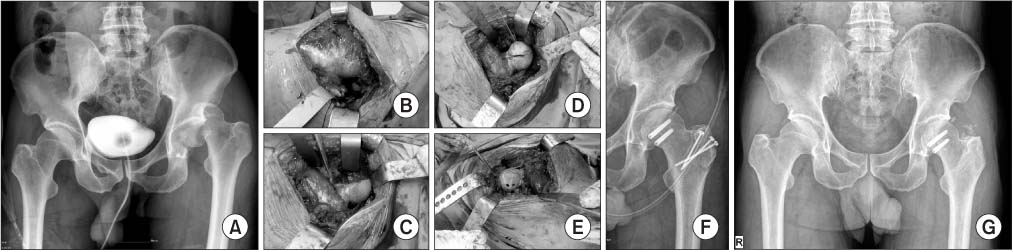
Figure 4 (A) A 52-year-old male had a left hip dislocation with Pipkin type II femoral head fracture. (B) Failed reduction resulted in an emergency open reduction and internal fixation. A photo showed a posteriorly dislocated femoral head. (C) After surgical dislocation, the left femoral head and neck were exposed. (D) After anatomical reduction, provisionary K-wires were fixed. (E) Internal fixation with headless screws was performed. (F) Postoperative X-ray showing anatomical reduction and congruent hip. (G) Two-year-follow up X-ray demonstrating mild heterotopic ossification, but no evidence of osteonecrosis of the femoral head or arthritis.
Reference
-
1. Kim JW, Chung HW, Jeon TS, Shim HN, Yoon TY, Kim YC. Traumatic femoral head fracture without hip dislocation: a case report. Hip Pelvis. 2012; 24:256–260.2. Brumback RJ, Kenzora JE, Levitt LE, Burgess AR, Poka A. Fractures of the femoral head. Hip. 1987; 181–206.3. Butler JE. Pipkin Type-II fractures of the femoral head. J Bone Joint Surg Am. 1981; 63:1292–1296.
Article4. Hougaard K, Thomsen PB. Coxarthrosis following traumatic posterior dislocation of the hip. J Bone Joint Surg Am. 1987; 69:679–683.
Article5. Epstein HC, Wiss DA, Cozen L. Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res. 1985; 201:9–17.
Article6. Suraci AJ. Distribution and severity of injuries associated with hip dislocations secondary to motor vehicle accidents. J Trauma. 1986; 26:458–460.
Article7. Droll KP, Broekhuyse H, O'Brien P. Fracture of the femoral head. J Am Acad Orthop Surg. 2007; 15:716–727.
Article8. Pipkin G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am. 1957; 39:1027–1042 passim.
Article9. Roeder LF Jr, DeLee JC. Femoral head fractures associated with posterior hip dislocation. Clin Orthop Relat Res. 1980; 147:121–130.10. Browner BD, Jupitor J, Levine A, Trafton P. Skeletal trauma: basic science, management, and reconstruction. Philadelphia: Saunders;2003. p. 1657–1690.11. Stannard JP, Harris HW, Volgas DA, Alonso JE. Functional outcome of patients with femoral head fractures associated with hip dislocations. Clin Orthop Relat Res. 2000; 377:44–56.
Article12. Swiontkowski MF, Thorpe M, Seiler JG, Hansen ST. Operative management of displaced femoral head fractures: casematched comparison of anterior versus posterior approaches for Pipkin I and Pipkin II fractures. J Orthop Trauma. 1992; 6:437–442.13. Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001; 83:1119–1124.14. Kloen P, Siebenrock KA, Raaymakers ELFB, Marti RK, Ganz R. Femoral head fractures revisited. Eur J Trauma. 2002; 28:221–233.
Article15. Massè A, Aprato A, Alluto C, Favuto M, Ganz R. Surgical hip dislocation is a reliable approach for treatment of femoral head fractures. Clin Orthop Relat Res. 2015; 05. 21. Published online.
Article16. Keene GS, Villar RN. Arthroscopic loose body retrieval following traumatic hip dislocation. Injury. 1994; 25:507–510.
Article17. Svoboda SJ, Williams DM, Murphy KP. Hip arthroscopy for osteochondral loose body removal after a posterior hip dislocation. Arthroscopy. 2003; 19:777–781.
Article18. Park MS, Her IS, Cho HM, Chung YY. Internal fixation of femoral head fractures (Pipkin I) using hip arthroscopy. Knee Surg Sports Traumatol Arthrosc. 2014; 22:898–901.
Article19. Marchetti ME, Steinberg GG, Coumas JM. Intermediateterm experience of Pipkin fracture-dislocations of the hip. J Orthop Trauma. 1996; 10:455–461.
Article20. Kim JW, Chang JS, Bae JY, Kim JJ. Outcomes of treatment for femoral head fractures with hip dislocation: review of 20 cases. J Korean Hip Soc. 2010; 22:298–304.21. Park KS, Lee KB, Na BR, Yoon TR. Clinical and radiographic outcomes of femoral head fractures: excision vs. fixation of fragment in Pipkin type I: what is the optimal choice for femoral head fracture? J Orthop Sci. 2015; 05. 08. Published online. DOI: 10.1007/s00776-015-0732-6.
Article22. Bartlett CS 3rd, Birch CE. Femoral head reduction osteoplasty for fracture dislocation: a surgical technique. Injury. 2015; 03. 10. Published online. DOI: 10.1016/j.injury.2015.03.003.
Article23. Gagała J, Tarczyńska M, Gawęda K. Fixation of femoral head fractures with autologous osteochondral transfer (mosaicplasty). J Orthop Trauma. 2014; 28:e226–e230.
Article24. Yang KH. Principles of fracture management. . Seoul: Panmun Education;2013. p. 581–592. .25. Hillyard RF, Fox J. Sciatic nerve injuries associated with traumatic posterior hip dislocations. Am J Emerg Med. 2003; 21:545–548.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Femoral Head and Neck Fractures developed in Avascular Necrosis of the Femoral Head
- Surgical Treatment of the Atypical Femoral Fracture: Overcoming Femoral Bowing
- Early Detection of Viability of the Femoral Head by 99mTc-MDP Bone Scan in Femoral Neck Fracture
- Chordoma in the Femoral Head and Gluteus Maximus Muscle: A Case Report
- Treatment of intertrochanteric fractures with bipolar hemiarthroplasty in the elderly
