Below the Knee Intervention Using Multidisciplinary Methods Including an Antegrade, Retrograde Approach Without the Use of a Sheath but With a Plaque Excision Device
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Gwangju Veterans Hospital, Gwangju, Korea. gpkwy@naver.com
- 2Division of Cardiology, Department of Internal Medicine, Kyung Hee University College of Medicne, Seoul, Korea.
- KMID: 1826386
- DOI: http://doi.org/10.4070/kcj.2012.42.2.125
Abstract
- Below the knee (BTK) interventions are increasing in patients with rest pain or critical limb ischemia, and these interventions are frequently successful in facilitating limb salvage. New intervention techniques and devices allow successful recanalization of occluded BTK arteries. Here, we report a case of successful recanalization of BTK arteries using multidisciplinary methods, including an antegrade approach and retrograde approach without the use of a sheath, but with simple balloon angioplasty, and plaque excision using Silverhawk atherectomy device.
Keyword
MeSH Terms
Figure
-

Fig. 1 Computed tomography and angioplasty of the lower extremities. A: computed tomography with contrast revealed diffuse significant arterial stenosis in the left proximal to mid superficial femoral artery, total occlusion in the left distal SFA, diffuse arterial stenosis in the left popliteal artery, and total occlusion of the left tibioperoneal trunk. B, C, and D: angiography revealed a patent left proximal SFA with total occlusion of the left distal SFA to the popliteal artery with a poor distal run-off vessel. SFA: superficial femoral artery.
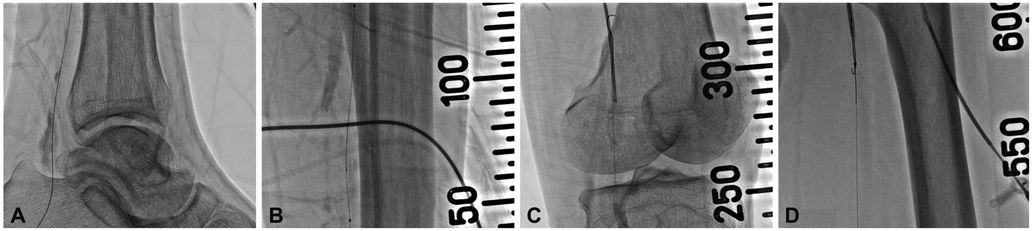
Fig. 2 Wire passage via the posterior tibial artery. A: the left pedal artery was punctured using an 18 gauge Seldinger needle and the wire was advanced successfully. B: after advancing the wire up to the tibioperoneal trunk, a 3×100 mm Savvy balloon was placed, without ballooning, as a sheath substitute. C and D: after successfully crossing the wire, we pulled the wire via a right femoral sheath using a snare (10 mm, pfm Produkte fur die Medizin AG).
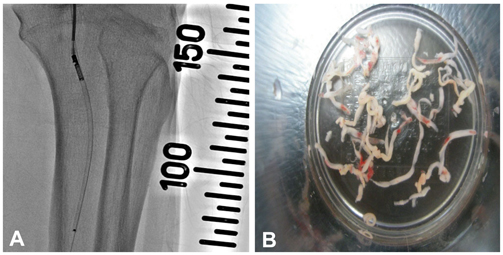
Fig. 3 Percutaneous transluminal angioplasty and plaque excision. A: we performed PTA in the left popliteal artery using a 3×100 mm Savvy balloon at 6-10 atm. B: plaque excision using the Silverhawk device.

Fig. 4 Final angiography demonstrated a good distal flow without residual stenosis.
Reference
-
1. Staffa R, Leypold J, Vojtísek B. Pedal bypass versus PTA (percutaneous transluminal angioplasty) of the crural arteries. Rozhl Chir. 2003. 82:516–521.2. Adam DJ, Beard JD, Cleveland T, et al. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet. 2005. 366:1925–1934.3. Faglia E, Dalla Paola L, Clerici G, et al. Peripheral angioplasty as the first-choice revascularization procedure in diabetic patients with critical limb ischemia: prospective study of 993 consecutive patients hospitalized and followed between 1999 and 2003. Eur J Vasc Endovasc Surg. 2005. 29:620–627.4. Saito S. Different strategies of retrograde approach in coronary angioplasty for chronic total occlusion. Catheter Cardiovasc Interv. 2008. 71:8–19.5. Fusaro M, Dalla Paola L, Biondi-Zoccai GG. Retrograde posterior tibial artery access for below-the-knee percutaneous revascularization by means of sheathless approach and double wire technique. Minerva Cardioangiol. 2006. 54:773–777.6. Keeling WB, Shames ML, Stone PA, et al. Plaque excision with the Silverhawk catheter: early results in patients with claudication or critical limb ischemia. J Vasc Surg. 2007. 45:25–31.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Iteration of Reverse Controlled Antegrade and Retrograde Tracking for Coronary Chronic Total Occlusion Intervention: a Current Appraisal
- Lateral Lithotomy Position for Simultaneous Retrograde and Antegrade Approach to the Ureter
- Arthrodesis of the Knee Using a Retrograde Femoral Intramedullary Nail: Technical Report
- Anterior Tibial Artery Angioplasty and Stenting by Retrograde Pedal Artery Approach in Diabetic Patient with Critical Limb Ischemia: A Case Report
- Recanalization of a Coronary Chronic Total Occlusion by a Retrograde Approach Using Ipsilateral Double Guiding Catheters
