Successful Treatment of a Ruptured Aortic Arch Aneurysm Using a Hybrid Procedure
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Medical Research Institute, Pusan National University Hospital, Busan, Korea. glaraone@hanmail.net
- 2Department of Thoracic and Cardiovascular Surgery, Medical Research Institute, Pusan National University Hospital, Busan, Korea.
- KMID: 1826355
- DOI: http://doi.org/10.4070/kcj.2011.41.8.469
Abstract
- Aortic rupture has a high mortality rate and can be considered a medical emergency. The standard treatment for aortic rupture is surgical repair. An aortic stent graft for a ruptured descending aorta is considered an effective alternative treatment. However, an aortic stent graft is difficult when the aortic aneurysm is in the aortic arch due to supra-aortic vessels. We report on a patient with a ruptured aortic arch aneurysm treated with a hybrid procedure, which involved a carotid to carotid bypass operation and an aortic stent graft. A 71-year-old male patient visited our cardiovascular center suffering from hemoptysis. The chest CT and aortography showed a 9 cm sized aortic arch aneurysm 0.5 cm distal to the left subclavian artery and a hemothorax in the left lung. The patient refused to undergo a full open operation. We performed a carotid to carotid bypass in advance, and two pieces of aortic stent grafts were placed across the left carotid artery and left subclavian artery. The follow up CT showed the aortic stent grafts, no endoleaks and no thrombus in the aortic arch aneurysm. The patient was discharged from the hospital without complication.
Keyword
MeSH Terms
Figure
-
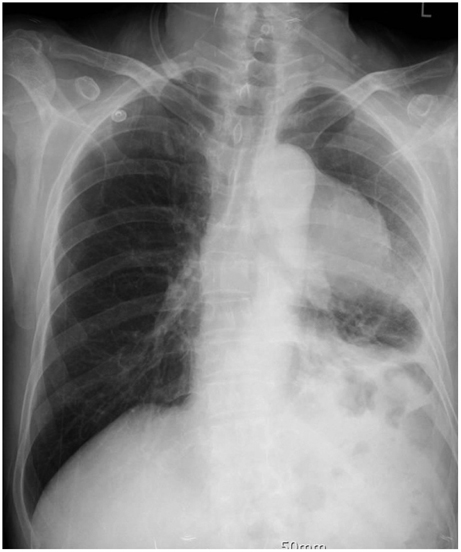
Fig. 1 The chest X-ray shows a mass-like lesion in the left hilar zone.
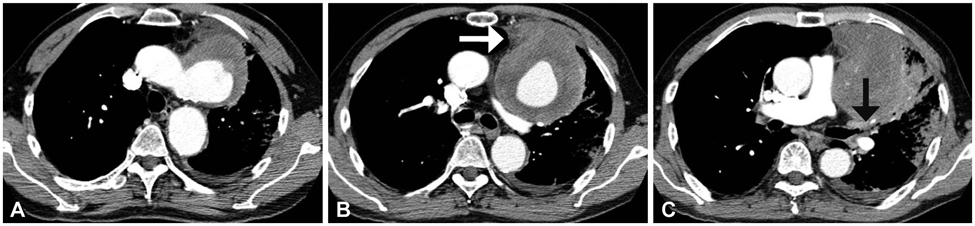
Fig. 2 The chest CT scan shows a saccular aneurysm with intramural thrombus in the aortic arch (A). The aortic aneurysm is suspected to be leaking to the anterior chest wall (white arrow) (B) and the left main bronchus is compressed by the huge aortic aneurysm (black arrow) (C).

Fig. 3 Aortography shows a huge aortic arch aneurysm 0.2 cm distal to the left subclavian artery (A) and the process of deploying 2 pieces of aortic stent grafts (40 mm×10 cm, 36 mm×10 cm, S&G biotech, Korea) across the left carotid artery and left subclavian artery (B, C and D).

Fig. 4 The chest X-ray shows total atelectasis of the left lung (A). The left main bronchus is compressed due to the posteriorly displaced left pulmonary artery, resulting in left lung total atelectasis on the chest CT scan (black arrow) (B) and there is no endoleak or occlusion of the neck vessels (C).

Fig. 5 The chest X-ray shows the improvement of the left atelectasis 7 days after bronchoscopy (A) and the follow up CT scan shows the aortic stent grafts, no endoleak and no thrombus in the aortic arch aneurysm (B and C).
Reference
-
1. Clouse WD, Hallett JW Jr, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ 3rd. Improved prognosis of thoracic aortic aneurysm: a population-based study. JAMA. 1998. 280:1926–1929.2. Kouchoukos NT, Dougenis D. Surgery of the thoracic aorta. N Engl J Med. 1997. 336:1876–1888.3. Dake MD. Endovascular stent-graft management of thoracic aortic diseases. Eur J Radiol. 2001. 39:42–49.4. Dake MD, Miller DC, Semba CP, Mitchell RS, Walker PJ, Liddell RP. Transluminal placement of endovascular stent-grafts for the treatment of descending thoracic aortic aneurysms. N Engl J Med. 1994. 331:1729–1734.5. Criado FJ, Barnatan MF, Rizk Y, Clark NS, Wang CF. Technical st-rategies to expand stent-graft applicability in the aortic arch and pro-ximal descending thoracic aorta. J Endovasc Ther. 2002. 9:Suppl 2. II32–II38.6. Czerny M, Fleck T, Zimpfer D, et al. Combined repair of an aortic arch aneurysm by sequential transposition of the supra-aortic branches and endovascular stent-graft placement. J Thorac Cardiovasc Surg. 2003. 126:916–918.7. Halperin JL, Olin JW. Fuster V, editor. Disease of the aorta. Hurst's The Heart. 2004. 11th ed. New York: McGraw-Hil;2304.8. Cohn PF, Braunwald E. Braunwald E, editor. Disease of the aorta. Heart Disease. 1997. 5th ed. Philadelphia: Saunders;1550.9. Johansson G, Markstrom U, Swedenborg J. Ruptured thoracic aortic aneurysms: a study of incidence and mortality rates. J Vasc Surg. 1995. 21:985–988.10. Sunder-Plassmann L, Scharrer-Pamler R, Liewald F, Kapfer X, Gorich J, Orend KH. Endovascular exclusion of thoracic arotic aneurysm: mid-term results of elective treatment and in contained rupture. J Card Surg. 2003. 18:367–374.11. Hausegger KA, Oberwaldner P, Tiesenhausen K, et al. Intentional left subclavian artery occlusion by thoracic aortic stent-grafts without surgical transposition. J Endovasc Ther. 2001. 8:472–476.12. Zipfel B, Buz S, Hammerschmidt R, Hetzer R. Occlusion of the left subclavian artery with stent grafts is safer with protective reconstruction. Ann Thorac Surg. 2009. 88:498–505.13. Killen DA, Muehlebach GF, Wathanacharoen S. Aortopulmonary fistula. South Med J. 2000. 93:195–198.14. Favre J, Gournier J, Adham M, Rosset E, Barral X. Aortobronchial fistula: report of three cases and review of the literature. Surgery. 1994. 115:264–270.15. Kim SE, Kim HJ, Lee SH, et al. A case of aortopulmonary fistula caused by a huge thoracic aortic aneurysm. Korean Circ J. 2009. 39:209–212.16. Nishizawa J, Matsumoto M, Sugita T, et al. Surgical treatment of five patients with aortobronchial fistula in the aortic arch. Ann Thorac Surg. 2004. 77:1821–1823.17. Kochi K, Okada K, Watari M, Orihashi K, Sueda T. Hybrid endovascu-lar stent grafting for aortic arch aneurysm with aortopulmonary fistula. J Thorac Cardiovasc Surg. 2002. 123:363–364.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hybrid Method for Stent-graft Insertion in a Patient with a Thoracic Aortic Aneurysm Involving the Aortic Arch: A case report
- Hybrid Procedure for Aortic Arch Repair: Arch Vessels Debranching with Supraaortic Revascularization Followed by Endovascular Aortic Stent Grafting
- Hybrid Procedure for Aortic Arch Aneurysm: Arch Vessels Debranching and Thoracic Endovascular Aortic Repair?: 2 case reports
- Visceral Debranching Thoracic Endovascular Aneurysm Repair for Chronic Dissecting Thoracoabdominal Aortic Aneurysm
- General Considerations of Ruptured Abdominal Aortic Aneurysm: Ruptured Abdominal Aortic Aneurysm
