J Korean Surg Soc.
2012 Aug;83(2):88-91. 10.4174/jkss.2012.83.2.88.
Routine barium enema prior to closure of defunctioning ileostomy is not necessary
- Affiliations
-
- 1Department of Surgery, Ajou University School of Medicine, Suwon, Korea. kgsosy@ajou.ac.kr
- KMID: 1820092
- DOI: http://doi.org/10.4174/jkss.2012.83.2.88
Abstract
- PURPOSE
The use of barium enemas to confirm the anastomotic integrity prior to ileostomy closure is still controversial. The purpose of the study was to determine the utility of routine contrast enema prior to ileostomy closure and its impact on patient management in patients with a low pelvic anastomosis.
METHODS
One hundred forty-five patients had a temporary loop ileostomy constructed to protect a low colorectal or coloanal anastomosis following low anterior resection for rectal cancer. All patients were evaluated by physical examination, proctoscopy, and barium enema prior to ileostomy closure.
RESULTS
The median time from ileostomy creation to closure was 8 months. Five (3.5%) of the 144 patients were found to have clinically relevant strictures at the colorectal anastomosis on routine barium enema. One patient (0.7%) showed anastomotic leak on their barium enema. Overall, 141 patients (97.9%) had an uncomplicated postoperative course. Postoperative complication occurred in three patients (2.1%). None of them showed abnormal barium enema finding, which suggested that routine contrast enema examination did not predict postoperative complication.
CONCLUSION
Routine barium enema evaluation of low pelvic anastomoses before loop ileostomy closure did not provide any additional information for postoperative colorectal anastomotic complication.
MeSH Terms
Figure
-
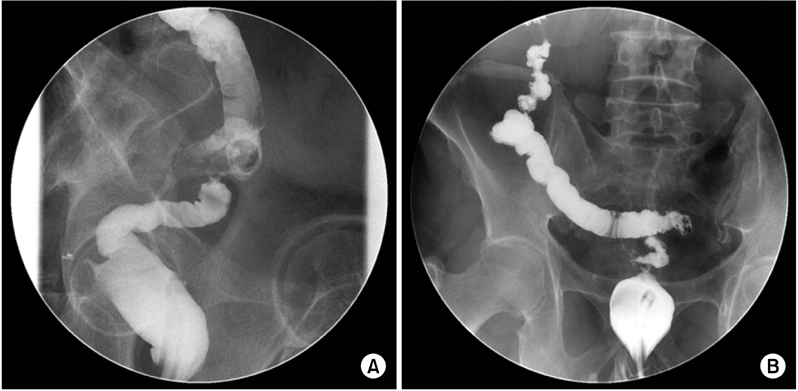
Fig. 1 (A) A 64-year-old man with stricture at colorectal anastomosis after low anterior resection for rectal cancer. (B) A 52-year-old man with fistula at rectal stump after low anterior resection for rectal cancer.
Reference
-
1. MacFarlane JK, Ryall RD, Heald RJ. Mesorectal excision for rectal cancer. Lancet. 1993. 341:457–460.2. Williams N, Seow-Choen F. Physiological and functional outcome following ultra-low anterior resection with colon pouch-anal anastomosis. Br J Surg. 1998. 85:1029–1035.3. Karanjia ND, Corder AP, Bearn P, Heald RJ. Leakage from stapled low anastomosis after total mesorectal excision for carcinoma of the rectum. Br J Surg. 1994. 81:1224–1226.4. Arbman G, Nilsson E, Hallbook O, Sjodahl R. Local recurrence following total mesorectal excision for rectal cancer. Br J Surg. 1996. 83:375–379.5. Horgan AF, Finlay IG. Preoperative staging of rectal cancer allows selection of patients for preoperative radiotherapy. Br J Surg. 2000. 87:575–579.6. Wheeler JM, Gilbert JM. Controlled intraoperative water testing of left-sided colorectal anastomoses: are ileostomies avoidable? Ann R Coll Surg Engl. 1999. 81:105–108.7. Tan WS, Tang CL, Shi L, Eu KW. Meta-analysis of defunctioning stomas in low anterior resection for rectal cancer. Br J Surg. 2009. 96:462–472.8. Khair G, Alhamarneh O, Avery J, Cast J, Gunn J, Monson JR, et al. Routine use of gastrograffin enema prior to the reversal of a loop ileostomy. Dig Surg. 2007. 24:338–341.9. MacLeod I, Watson AJ, Hampton J, Hussey JK, O'Kelly TJ. Colonic pouchography is not routinely required prior to stoma closure. Colorectal Dis. 2004. 6:162–164.10. Dolinsky D, Levine MS, Rubesin SE, Laufer I, Rombeau JL. Utility of contrast enema for detecting anastomotic strictures after total proctocolectomy and ileal pouch-anal anastomosis. AJR Am J Roentgenol. 2007. 189:25–29.11. da Silva GM, Wexner SD, Gurland B, Gervaz P, Moon SD, Efron J, et al. Is routine pouchogram prior to ileostomy closure in colonic J-pouch really necessary? Colorectal Dis. 2004. 6:117–120.12. Brown JJ, Balfe DM, Heiken JP, Becker JM, Soper NJ. Ileal J pouch: radiologic evaluation in patients with and without postoperative infectious complications. Radiology. 1990. 174:115–120.13. Thoeni RF, Fell SC, Engelstad B, Schrock TB. Ileoanal pouches: comparison of CT, scintigraphy, and contrast enemas for diagnosing postsurgical complications. AJR Am J Roentgenol. 1990. 154:73–78.14. Gelfand DW. Complications of gastrointestinal radiologic procedures: I. Complications of routine fluoroscopic studies. Gastrointest Radiol. 1980. 5:293–315.15. Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, et al. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004. 32:858–873.16. Lee MR, Lee MJ, Kim JH, Hwang Y. Is barium enema prior to ileostomy closure necessary? J Korean Soc Coloproctol. 2006. 22:298–300.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Is Barium Enema Prior to Ileostomy Closure Necessary?
- Enterogastroesophageal reflux during barium enema : report of a case
- Reduction rate and influencing factors of intussusception by hydrostatic water enema under ultrasound guidance and barium enema
- Diagnostic value of barium enema in acute appendicitis
- The diagnostic value of barium enema in acute appendicitis
