J Korean Surg Soc.
2011 Apr;80(4):267-271. 10.4174/jkss.2011.80.4.267.
Gynecologic pathologies in our appendectomy series and literature review
- Affiliations
-
- 1Department of Surgery, Izmir Bozyaka Training and Research Hospital, Izmir, Turkey. omerengin@hotmail.com
- 2Department of Surgery, Buca Seyfi Demirsoy Large State Hospital, Izmir, Turkey.
- 3Department of Pathology, Buca Seyfi Demirsoy Large State Hospital, Izmir, Turkey.
- KMID: 1820017
- DOI: http://doi.org/10.4174/jkss.2011.80.4.267
Abstract
- PURPOSE
Appendectomy applied from the diagnosis of acute appendicitis is one the most common operations in surgery. The rates of negative appendectomy are still high. The rates of negative appendectomy in males and females differ and are higher in females. In our study, these differences, particularly in females, were studied and possible solutions were discussed.
METHODS
Between October 2002 and October 2009, among women receiving urgent appendectomies, those whose primary cause was gynecological pathology were studied retrospectively. All our women subjects were examined by preoperative gynecologists. After gynecological consultation, the patients were evaluated by a general surgeon due to lack of urgent ultrasonography, computed tomography (CT) and diagnostic laparoscopy and the patient received appendectomy due to acute appendicitis.
RESULTS
In our series of 1,969 appendectomies, the rate of female/male is 811/1,158. It was determined that the primary cause in 47 (47/811; 5.8%) women with applied appendectomy was gynecological pathology. As a gynecological pathology, it was observed that the most common cause was ovarian cyst ruptures at a rate of 72.3%. The negative appendectomy rate in males was found to be 14.94% (173/1,158), and in females it was 22.56% (183/811). The difference between them is significant (P < 0.01). Of these women, 5.8% were gynecologically-induced and 16.76% were unrelated to gynecological causes.
CONCLUSION
We believe that gynecological consultation before appendectomy in women is necessary, but not sufficient. It is also important that at least one of the facilities, such as us, CT, magnetic resonance imaging, and diagnostic laparoscopy should be available in surgical use for the diagnosis of negative appendicitis.
MeSH Terms
Figure
-
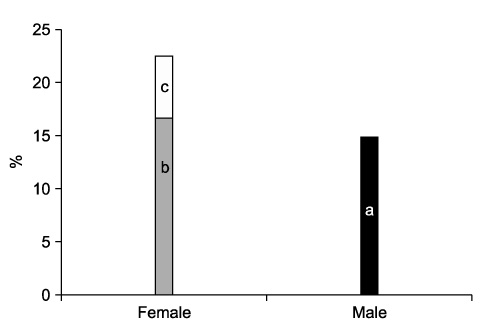
Fig. 1 Negative appendectomy. a, negative appendectomy in males; b, the causes of gynecology in females having negative appendectomy; c, gynecologic causes in females having negative appendectomy.
Reference
-
1. Osime O, Ajayi P. Incidence of negative appendectomy: experience from a company hospital in Nigeria. Cal J Emerg Med. 2005. 6:69–73.2. Ertekin C, Guloğlu R, Taviloglu K. Acil cerrahi. 2009. Istanbul: Nobel Tıp Kitabevleri;301–317.3. Townsend CM, Beauchamp RD, Evers BM, Mattox KL. Sabiston textbook of surgery. 2004. 17th ed. Philadelphia: Saunders;1381–1397.4. Zinner MJ, Ashley SW. Maingot's abdominal operations. 2007. 11th ed. NewYork: McGraw-Hill;589–611.5. Sayek I. Temel Cerrahi. 2004. Ankara: Güneş Kitabevi;1191–1197.6. Huwart L, El Khoury M, Lesavre A, Phan C, Rangheard AS, Bessoud B, et al. Is appendicolith a reliable sign for acute appendicitis at MDCT? J Radiol. 2006. 87(4 Pt 1):383–387.7. Turan YH, Kalyoncu S, Boran N, Gungor M, Demirel LC, Ortac F. Concurrent appendectomy in gynecologic surgery. T Klin Jînekol Obst. 1994. 4:190–192.8. Pieper R, Kager L, Tidefeldt U. Obstruction of appendix vermiformis causing acute appendicitis. An experimental study in the rabbit. Acta Chir Scand. 1982. 148:63–72.9. Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986. 15:557–564.10. Wente MN, Waleczek H. Strategy for avoidance of negative appendectomies. Chirurg. 2009. 80:588–593.11. Chooi WK, Brown JA, Zetler P, Wiseman S, Cooperberg P. Imaging of acute appendicitis and its impact on negative appendectomy and perforation rates: the St. Paul's experience. Can Assoc Radiol J. 2007. 58:220–224.12. Binnebösel M, Otto J, Stumpf M, Mahnken AH, Gassler N, Schumpelick V, et al. Acute appendicitis. Modern diagnostics--surgical ultrasound. Chirurg. 2009. 80:579–587.13. Rao PM, Rhea JT, Rattner DW, Venus LG, Novelline RA. Introduction of appendiceal CT: impact on negative appendectomy and appendiceal perforation rates. Ann Surg. 1999. 229:344–349.14. Lim GH, Shabbir A, So JB. Diagnostic laparoscopy in the evaluation of right lower abdominal pain: a one-year audit. Singapore Med J. 2008. 49:451–453.15. van den Broek WT, Bijnen AB, de Ruiter P, Gouma DJ. A normal appendix found during diagnostic laparoscopy should not be removed. Br J Surg. 2001. 88:251–254.16. Townsend CM, Beauchamp RD, Evers BM, Mattox KL. Sabiston textbook of surgery. 2004. 17th ed. Philadelphia: Saunders;2255.17. Styrud J, Eriksson S, Granström L. Treatment of perforated appendicitis: an analysis of 362 patients treated during 8 years. Dig Surg. 1998. 15:683–686.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Laparoscopic and Open Appendectomies
- The Benefits and Risks of Performing Incidental Appendectomy
- Comparison between an Interval Appendectomy and an Urgent Appendectomy for Patients of Periappendiceal Abscess
- A Case of Endometriosis in Appendectomy Scar
- Incidental Appendectomy During Gynecologic Laparoscopic Surgery
