Gallbladder Wall Thickening and Periportal Tracking on CT in Patients with Acute Pyelonephritis
- Affiliations
-
- 1Department of Radiology, Anam Hospital, Korea University College of Medicine, Seoul, Korea. urorad@korea.ac.kr
- KMID: 1819753
- DOI: http://doi.org/10.3348/jksr.2012.67.5.381
Abstract
- PURPOSE
To assess gallbladder (GB) wall thickening and periportal tracking on CT in patients with acute pyelonephritis (APN) by each kidney involvement.
MATERIALS AND METHODS
A total of 117 patients diagnosed with APN by clinical examination and CT were included in this retrospective study. The patients were divided into three groups based on kidney involvement seen on CT: right APN, left APN, and bilateral APN. Two radiologists reviewed CT images in consensus for the presence of diffuse GB wall thickening and periportal tracking. The prevalence of these two manifestations was compared among the three groups.
RESULTS
The prevalence of GB wall thickening in patients with right APN (26.4%) and bilateral APN (19%) was significantly higher than in patients with left APN (0%) (p < 0.016). The prevalence of periportal tracking in patients with right APN (15.1%) and bilateral APN (26%) was higher than in patients with left APN (3%), with a significant difference between patients with bilateral APN and left APN (p < 0.016).
CONCLUSION
GB wall thickening and periportal tracking are predominantly encountered on CT in patients with APN involving the right kidney (right and bilateral APN), and should be considered in differential diagnosis of diseases associated with GB wall thickening and periportal tracking.
MeSH Terms
Figure
-
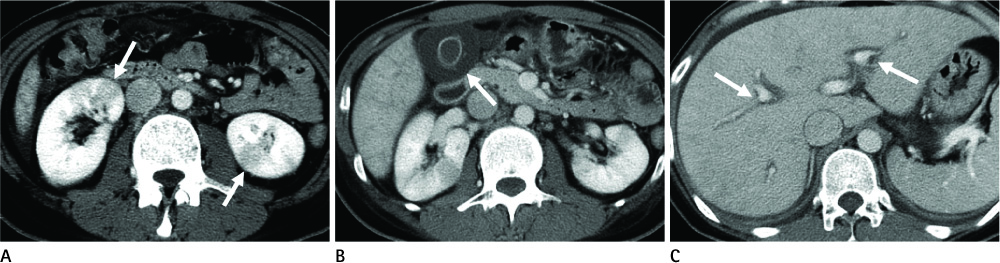
Fig. 1 A 36-year-old woman with fever and bilateral flank pain. A. Axial contrast-enhanced CT scan demonstrates wedge shaped hypoattenuating area within the bilateral kidneys (arrows), features consistent with bilateral APN. B, C. CT scans show thick-walled GB that contains hypodense outer layer corresponding to subserosal edema (arrow in B) and periportal tracking (arrows in C) in the liver. Note.-APN = acute pyelonephritis, GB = gallbladder
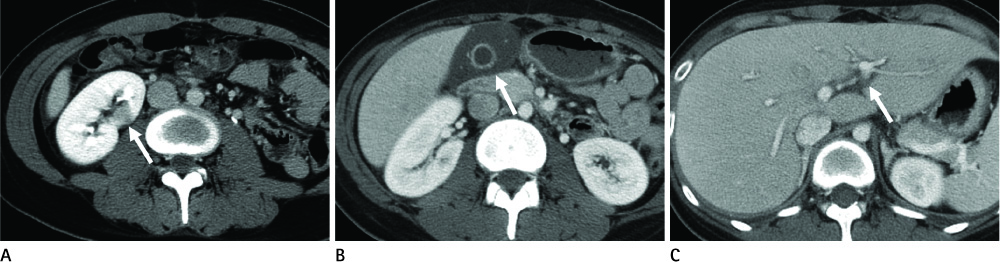
Fig. 2 A 22-year-old woman with right flank pain. A. Axial contrast-enhanced CT scan demonstrates wedge shaped hypoattenuating area within right kidney (arrow), features consistent with right APN. B, C. CT scans show edematous GB wall thickening (arrow in B) and periportal tracking (arrow in C) in the liver. Note.-APN = acute pyelonephritis, GB = gallbladder
Reference
-
1. Zissin R, Osadchy A, Shapiro-Feinberg M, Gayer G. CT of a thickened-wall gall bladder. Br J Radiol. 2003. 76:137–143.2. Aspestrand F, Schrumpf E, Jacobsen M, Hanssen L, Endresen K. Increased lymphatic flow from the liver in different intra- and extrahepatic diseases demonstrated by CT. J Comput Assist Tomogr. 1991. 15:550–554.3. Lawson TL, Thorsen MK, Erickson SJ, Perret RS, Quiroz FA, Foley WD. Periportal halo: a CT sign of liver disease. Abdom Imaging. 1993. 18:42–46.4. Zissin R, Osadchy A, Gayer G, Kitay-Cohen Y. Extrarenal manifestations of severe acute pyelonephritis: CT findings in 21 cases. Emerg Radiol. 2006. 13:73–77.5. Zissin R, Kots E, Rachmani R, Hadari R, Shapiro-Feinberg M. Hepatic periportal tracking associated with severe acute pyelonephritis. Abdom Imaging. 2000. 25:251–254.6. Talarico HP, Rubens D. Gallbladder wall thickening in acute pyelonephritis. J Clin Ultrasound. 1990. 18:653–657.7. Compos FA, Rosas GQ, Goldenberg D, Szarf G, D'Ippolito G. Acute pyelonephritis: frequency of findings in patients submitted to computer tomography. Radiol Bras. 2007. 40:309–314.8. Kawashima A, Sandler CM, Goldman SM, Raval BK, Fishman EK. CT of renal inflammatory disease. Radiographics. 1997. 17:851–866. discussion 867-868.9. Jung DC. Korean society of urogenital radiology. Infectious disease of kidney and urogenital tuberculosis. Urogenital radiology: urologic imaging. 2009. Seoul: Ilchokak;53–63.10. Stunell H, Buckley O, Feeney J, Geoghegan T, Browne RF, Torreggiani WC. Imaging of acute pyelonephritis in the adult. Eur Radiol. 2007. 17:1820–1828.11. Rabushka LS, Fishman EK, Goldman SM. Pictorial review: computed tomography of renal inflammatory disease. Urology. 1994. 44:473–480.12. Papanicolaou N, Pfister RC. Acute renal infections. Radiol Clin North Am. 1996. 34:965–995.13. Goldman SM. Acute and chronic urinary infection: present concepts and controversies. Urol Radiol. 1988. 10:17–24.14. Goldman SM, Fishman EK. Upper urinary tract infection: the current role of CT, ultrasound, and MRI. Semin Ultrasound CT MR. 1991. 12:335–360.15. van Breda Vriesman AC, Engelbrecht MR, Smithuis RH, Puylaert JB. Diffuse gallbladder wall thickening: differential diagnosis. AJR Am J Roentgenol. 2007. 188:495–501.16. Parker AE. Studies on the main posterior lymph channels of the abdomen and their connections with the lymphatics of the genitourinary system. Am J Anat. 1935. 56:409.17. Deimer EE. Herlinger H, Lunderquist A, Wallace S, editors. Lymphatic anatomy. Clinical radiology of the liver. 1983. New York: Marcel Dekker;55–63.18. Ito M, Mishima Y. Lymphatic drainage of the gallbladder. J Hepatobiliary Pancreat Surg. 1994. 1:302–308.19. Freedland SJ, Dekernion JB. Role of lymphadenectomy for patients undergoing radical nephrectomy for renal cell carcinoma. Rev Urol. 2003. 5:191–195.20. Majd M, Nussbaum Blask AR, Markle BM, Shalaby-Rana E, Pohl HG, Park JS, et al. Acute pyelonephritis: comparison of diagnosis with 99mTc-DMSA, SPECT, spiral CT, MR imaging, and power Doppler US in an experimental pig model. Radiology. 2001. 218:101–108.21. Son JY, Kim YJ, Park HS, Yu NC, Ko SM, Jung SI, et al. Diffuse gallbladder wall thickening on computed tomography in patients with liver cirrhosis: correlation with clinical and laboratory variables. J Comput Assist Tomogr. 2011. 35:535–538.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adequate Management of Gallbladder Wall Thickening
- Acute Cholecystitis: Two-Phase Spiral CT Finding
- Intramural Hypoattenuated Nodules in Thickened Wall of the Gallbladder: CT Features According to Their Primary Causes
- Computed tomographic and ultrasound findings of gallbladder carcinoma
- Thickened Wall-Type GB Cancer and Complicated Cholecystitis: Comparison of CT Findings
