Bone Subtraction 3-Dimension CT Angiography Using 64-Slice Multidetector CT for the Evaluation of Steno-Occlusive Intra- and Extracranial Vascular Diseases: Comparison with Digital Subtraction Angiography
- Affiliations
-
- 1Department of Radiology, Gyeongsang National University School of Medicine, Jinju, Korea. choids@gnu.ac.kr
- 2Gyeongsang Institute of Health Science, Gyeongsang National University School of Medicine, Jinju, Korea.
- 3Department of Neurology, Gyeongsang National University School of Medicine, Jinju, Korea.
- 4Department of Radiology, Samsung Seoul Hospital, Seoul, Korea.
- KMID: 1819745
- DOI: http://doi.org/10.3348/jksr.2012.67.5.309
Abstract
- PURPOSE
To investigate the efficacy of bone subtraction CT angiography (BSCTA) for the evaluation of steno-occlusive intra- and extracranial vascular diseases.
MATERIALS AND METHODS
Fifty-six patients were examined using 64-slice multidetector CT and digital subtraction angiography (DSA). For BSCTA, both nonenhanced CT and enhanced CT angiography (CTA) data sets were obtained. The stenotic degree of each vascular segment was assessed and classified into 5 grades. With DSA as the standard, CTA images were compared.
RESULTS
For the evaluation of the extracranial vessels, 370 arterial segments were analyzed, and the stenotic degree revealed by CTA and DSA agreed in 359 (97.0%). There was a significant correlation between CTA and DSA (Rs = 0.974). For depiction of > or = 50% stenosis, the sensitivity, specificity, and diagnostic accuracy of BSCTA were 100%, 98.2%, and 98.6%, respectively. For the intracranial arteries, 1029 segments were analyzed, and CTA agreed with DSA in 966 (93.9%). There was a significant correlation between CTA and DSA for stenotic degree (Rs = 0.880). For the depiction of > or = 50% stenosis, the sensitivity, specificity, and diagnostic accuracy of CTA were 100%, 95.8%, and 96.0%, respectively. In all 74 segments of disagreement, the degree of stenosis was overestimated on CTA.
CONCLUSION
BSCTA is comparable to DSA for the evaluation of steno-occlusive intra- and extracranial vascular diseases. However, the stenotic degree tends to be overestimated on BSCTA, especially in cases of wall calcifications.
MeSH Terms
Figure
-

Fig. 1 A 75-year-old female patient with right MCA stenosis. Serial projection images of BSCTA show the entire neck and intracranial vessels with high quality. There is focal severe stenosis in M1 segment of the right MCA (arrow). Note.-BSCTA = bone subtraction CT angiography, MCA = middle cerebral artery
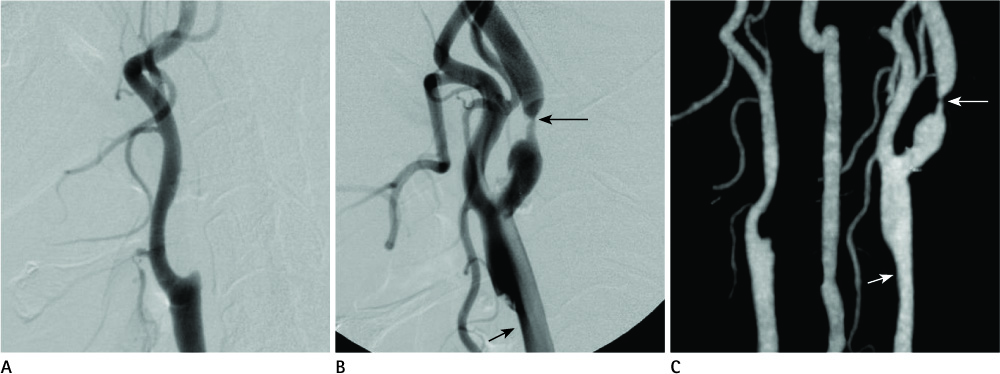
Fig. 2 A 65-year-old male patient with right ICA occlusion and left CCA and ICA stenosis. A. Lateral view of the right CCA angiogram shows complete occlusion of the right proximal ICA. B. Lateral view of the left CCA angiogram reveals mild segmental and severe focal narrowing in the left CCA (short arrow) and proximal ICA (long arrow). C. BSCTA also shows the lesions as the same as on DSA (long and short arrows). Note.-BSCTA = bone subtraction CT angiography, CCA = common carotid artery, DSA = digital subtraction angiography, ICA = internal carotid artery
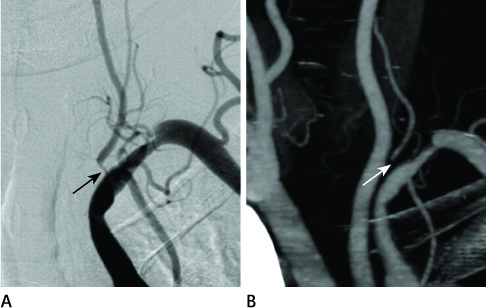
Fig. 3 A 67-year-old female patient with left proximal VA and subclavian artery stenosis. A. DSA shows severe and moderate degree stenosis in the left proximal VA (arrow) and subclavian artery. B. BSCTA reveals the stenotic lesions as the same degree as on DSA (arrow). Note.-BSCTA = bone subtraction CT angiography, DSA = digital subtraction angiography, VA = vertebral artery
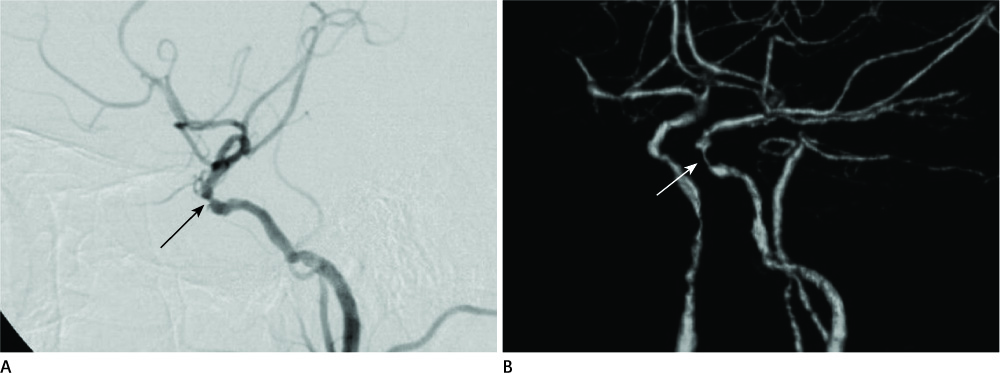
Fig. 4 A 59-year-old male patient with left cavernous ICA stenosis. A. DSA image shows focal luminal narrowing in the left cavernous ICA (arrow). B. On BSCTA, the stenotic lesion (arrow) is overestimated compared to DSA. Note.-BSCTA = bone subtraction CT angiography, DSA = digital subtraction angiography, ICA = internal carotid artery
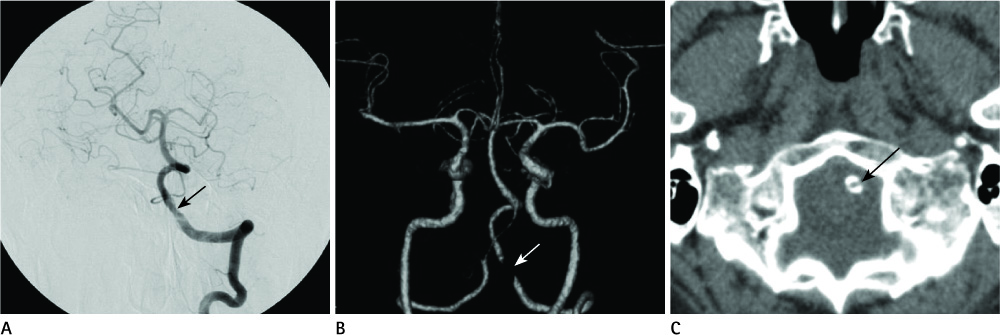
Fig. 5 A 65-year-old male patient with pseudostenosis. A. DSA of the left VA injection shows no significant stenosis without mild luminal irregularity in the left distal VA (arrow). B. On BSCTA, there is severe segmental narrowing in the left distal VA (arrow). C. NECT reveals circumferential calcification in the left distal VA (arrow). Note.-BSCTA = bone subtraction CT angiography, DSA = digital subtraction angiography, NECT = nonenhanced CT, VA = vertebral artery
Reference
-
1. Lell MM, Kramer M, Klotz E, Villablanca P, Ruehm SG. Carotid computed tomography angiography with automated bone suppression: a comparative study between dual energy and bone subtraction techniques. Invest Radiol. 2009. 44:322–328.2. Imakita S, Onishi Y, Hashimoto T, Motosugi S, Kuribayashi S, Takamiya M, et al. Subtraction CT angiography with controlled-orbit helical scanning for detection of intracranial aneurysms. AJNR Am J Neuroradiol. 1998. 19:291–295.3. Venema HW, Hulsmans FJ, den Heeten GJ. CT angiography of the circle of Willis and intracranial internal carotid arteries: maximum intensity projection with matched mask bone elimination-feasibility study. Radiology. 2001. 218:893–898.4. Siebert E, Bohner G, Dewey M, Bauknecht C, Klingebiel R. Dose related, comparative evaluation of a novel bone-subtraction algorithm in 64-row cervico-cranial CT angiography. Eur J Radiol. 2010. 73:168–174.5. Lell M, Anders K, Klotz E, Ditt H, Bautz W, Tomandl BF. Clinical evaluation of bone-subtraction CT angiography (BSCTA) in head and neck imaging. Eur Radiol. 2006. 16:889–897.6. Morhard D, Fink C, Becker C, Reiser MF, Nikolaou K. Value of automatic bone subtraction in cranial CT angiography: comparison of bone-subtracted vs. standard CT angiography in 100 patients. Eur Radiol. 2008. 18:974–982.7. Lell MM, Ruehm SG, Kramer M, Panknin C, Habibi R, Klotz E, et al. Cranial computed tomography angiography with automated bone subtraction: a feasibility study. Invest Radiol. 2009. 44:38–43.8. Randoux B, Marro B, Koskas F, Duyme M, Sahel M, Zouaoui A, et al. Carotid artery stenosis: prospective comparison of CT, three-dimensional gadolinium-enhanced MR, and conventional angiography. Radiology. 2001. 220:179–185.9. Samuels OB, Joseph GJ, Lynn MJ, Smith HA, Chimowitz MI. A standardized method for measuring intracranial arterial stenosis. AJNR Am J Neuroradiol. 2000. 21:643–646.10. Moll R, Dinkel HP. Value of the CT angiography in the diagnosis of common carotid artery bifurcation disease: CT angiography versus digital subtraction angiography and color flow Doppler. Eur J Radiol. 2001. 39:155–162.11. Bash S, Villablanca JP, Jahan R, Duckwiler G, Tillis M, Kidwell C, et al. Intracranial vascular stenosis and occlusive disease: evaluation with CT angiography, MR angiography, and digital subtraction angiography. AJNR Am J Neuroradiol. 2005. 26:1012–1021.12. Cumming MJ, Morrow IM. Carotid artery stenosis: a prospective comparison of CT angiography and conventional angiography. AJR Am J Roentgenol. 1994. 163:517–523.13. Leclerc X, Godefroy O, Pruvo JP, Leys D. Computed tomographic angiography for the evaluation of carotid artery stenosis. Stroke. 1995. 26:1577–1581.14. Schwartz RB, Jones KM, Chernoff DM, Mukherji SK, Khorasani R, Tice HM, et al. Common carotid artery bifurcation: evaluation with spiral CT. Work in progress. Radiology. 1992. 185:513–519.15. Khan S, Rich P, Clifton A, Markus HS. Noninvasive detection of vertebral artery stenosis: a comparison of contrast-enhanced MR angiography, CT angiography, and ultrasound. Stroke. 2009. 40:3499–3503.16. Khan S, Cloud GC, Kerry S, Markus HS. Imaging of vertebral artery stenosis: a systematic review. J Neurol Neurosurg Psychiatry. 2007. 78:1218–1225.17. Nguyen-Huynh MN, Wintermark M, English J, Lam J, Vittinghoff E, Smith WS, et al. How accurate is CT angiography in evaluating intracranial atherosclerotic disease? Stroke. 2008. 39:1184–1188.18. Hirai T, Korogi Y, Ono K, Nagano M, Maruoka K, Uemura S, et al. Prospective evaluation of suspected stenoocclusive disease of the intracranial artery: combined MR angiography and CT angiography compared with digital subtraction angiography. AJNR Am J Neuroradiol. 2002. 23:93–101.19. Buerke B, Puesken M, Wittkamp G, Stehling C, Ditt H, Seidensticker P, et al. Bone subtraction CTA for transcranial arteries: intra-individual comparison with standard CTA without bone subtraction and TOF-MRA. Clin Radiol. 2010. 65:440–446.20. Woodcock RJ Jr, Goldstein JH, Kallmes DF, Cloft HJ, Phillips CD. Angiographic correlation of CT calcification in the carotid siphon. AJNR Am J Neuroradiol. 1999. 20:495–499.21. Renker M, Nance JW Jr, Schoepf UJ, O'Brien TX, Zwerner PL, Meyer M, et al. Evaluation of heavily calcified vessels with coronary CT angiography: comparison of iterative and filtered back projection image reconstruction. Radiology. 2011. 260:390–399.22. Hegde A, Chan LL, Tan L, Illyyas M, Lim WE. Dual Energy CT and its use in neuroangiography. Ann Acad Med Singapore. 2009. 38:817–820.23. Watanabe Y, Uotani K, Nakazawa T, Higashi M, Yamada N, Hori Y, et al. Dual-energy direct bone removal CT angiography for evaluation of intracranial aneurysm or stenosis: comparison with conventional digital subtraction angiography. Eur Radiol. 2009. 19:1019–1024.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Assessment of Mesenteric Vascular Steno-occlusive Lesion in Acute Mesenteric Ischemia: Comparison between CT Angiography and Digital Subtraction Angiography
- Contrast-Enhanced Magnetic Resonance Angiography for Evaluation of the Steno-occlusive Disease of the Supraaortic Arteries: Comparison with Computed Tomography Angiography and Digital Subtraction Angiography
- Radiologic consideration of intra-arterial digital subtraction angiography
- Multidetector-Row CT Angiography of Cerebral Vasospasm after Aneurysmal Subarachnoid Hemorrhage: Comparison of Bone Subtraction and Standard CT Angiography with Digital Subtraction Angiography
- Multimodal Imaging Follow-up of a Thrombosed Developmental Venous Anomaly: CT, CT Angiography and Digital Subtraction Angiography
