Differential Diagnosis and Management of a Pituitary Mass with Renal Cell Carcinoma
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University College of Medicine, Seoul National University Hospital, Seoul, Korea. kimyh96@snu.ac.kr
- 2Department of Internal Medicine, Seoul National University College of Medicine, Seoul National University Hospital, Seoul, Korea.
- 3Department of Pathology, Seoul National University College of Medicine, Seoul National University Hospital, Seoul, Korea.
- KMID: 1814251
- DOI: http://doi.org/10.3340/jkns.2013.54.2.132
Abstract
- The small pituitary mass was incidentally found in 40-years-old women with renal cell carcinoma. The endocrinological and ophthalmological evaluation revealed no deficit and the short-term follow-up was recommended. In 6 months later, the visual disturbance was reported and the size of mass was increased. The tumor was removed totally via the trans-sphenoid approach. The post-operative endocrinological insufficiency was not noticed. During one year of follow-up period, there was no evidence of recurrence without adjuvant radiotherapy. The clinical features of pituitary metastasis from renal cell carcinoma were similar to those of pituitary adenoma. The possibility of pituitary metastasis should be kept in mind in patients with sellar mass and renal cell carcinoma.
Keyword
MeSH Terms
Figure
-
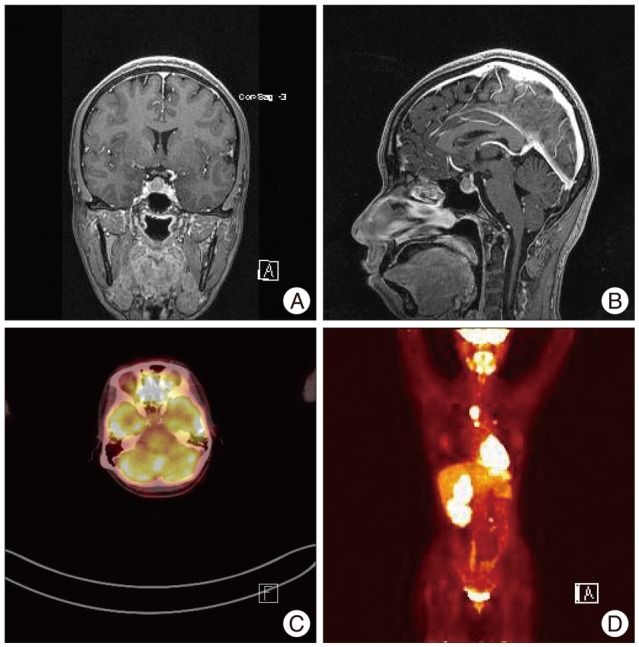
Fig. 1 The T1-weighted coronal (A) and sagittal (B) magnetic resonance images used to evaluate the intermittent headache reveal a round, well-enhanced sellar mass. The pituitary stalk is slightly deviated to the left by the tumor, and no optic compression is noted. 18F-fluorodeoxyglucose positron emission tomography shows no increased uptake in the sellar mass (C) in contrast to the other metastatic lesions in the body (D).
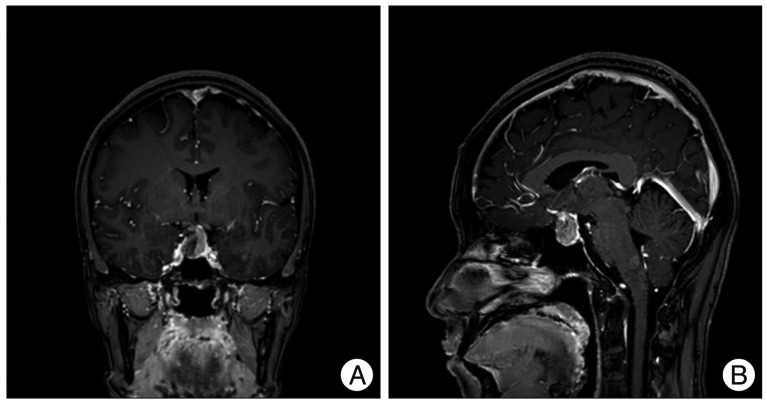
Fig. 2 The T1-weighted coronal (A) and sagittal (B) magnetic resonance images taken 6 months later show the markedly growing sellar mass compressing the optic chiasm.
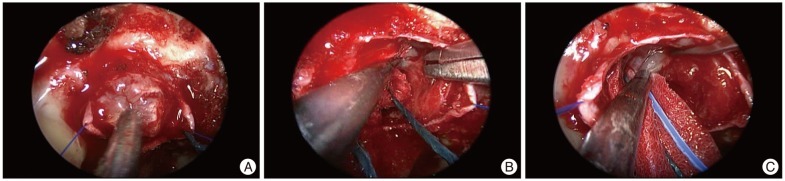
Fig. 3 The tumor was gray and moderately hard (A). It has a sharp margin between the pituitary gland (B) and the diaphragma sellae (C). The dissection plane between the tumor and the surrounding normal structures is not strongly adhesive.
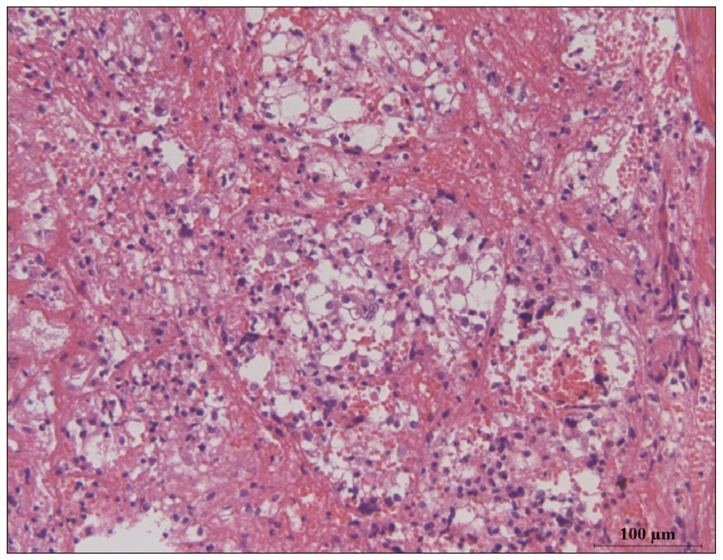
Fig. 4 The pathologic examination shows a nest of epithelial cells with clear cytoplasms and distinct cell membranes. The nests are separated by the highly vascularized stroma. Hematoxylin and eosin staining (×200).
Reference
-
1. Gopan T, Toms SA, Prayson RA, Suh JH, Hamrahian AH, Weil RJ. Symptomatic pituitary metastases from renal cell carcinoma. Pituitary. 2007; 10:251–259. PMID: 17541748.
Article2. Grossman R, Maimon S, Levite R, Ram Z. Multimodal treatment of hemorrhagic pituitary metastasis as first manifestation of renal cell carcinoma. World Neurosurg. 2013; 79:798.E1–798.E5. PMID: 22990000.
Article3. Hyun SH, Choi JY, Lee KH, Choe YS, Kim BT. Incidental focal 18F-FDG uptake in the pituitary gland : clinical significance and differential diagnostic criteria. J Nucl Med. 2011; 52:547–550. PMID: 21421711.
Article4. Kim YH, Lee BJ, Lee KJ, Cho JH. A case of pituitary metastasis from breast cancer that presented as left visual disturbance. J Korean Neurosurg Soc. 2012; 51:94–97. PMID: 22500201.
Article5. Komninos J, Vlassopoulou V, Protopapa D, Korfias S, Kontogeorgos G, Sakas DE, et al. Tumors metastatic to the pituitary gland : case report and literature review. J Clin Endocrinol Metab. 2004; 89:574–580. PMID: 14764764.
Article6. Kramer CK, Ferreira N, Silveiro SP, Gross JL, Dora JM, Azevedo MJ. Pituitary gland metastasis from renal cell carcinoma presented as a non-functioning macroadenoma. Arq Bras Endocrinol Metabol. 2010; 54:498–501. PMID: 20694412.
Article7. Max MB, Deck MD, Rottenberg DA. Pituitary metastasis : incidence in cancer patients and clinical differentiation from pituitary adenoma. Neurology. 1981; 31:998–1002. PMID: 7196526.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Renal Cell Carcinoma in Childhood
- Renal Cell Carcinoma in Children : Report of Two Cases
- A Case of Renal Oncocytoma with Synchronous Contralateral Renal Cell Carcinoma
- Cytologic Features of Renal Cell Carcinoma: Clear Cell, Granular Cell and Oncocytoma
- A Case of Pediatric Renal Cell Carcinoma with Multiple Hepatic Cyst
