Endovascular Treatment of Aneurysms Arising from the Proximal Segment of the Anterior Cerebral Artery
- Affiliations
-
- 1Department of Neurosurgery, Medical Research Institute, Pusan National University Hospital, Busan, Korea. medifirst@pusan.ac.kr
- 2Department of Diagnostic Radiology, Medical Research Institute, Pusan National University Hospital, Busan, Korea.
- 3Department of Neurosurgery, Medical Research Institute, Pusan National University Yangsan Hospital, Yangsan, Korea.
- KMID: 1814241
- DOI: http://doi.org/10.3340/jkns.2013.54.2.75
Abstract
OBJECTIVE
Aneurysms arising from the proximal segment of the anterior cerebral artery (A1) are rare and challenging to treat. The aim of this study was to report our experience with endovascular treatment of A1 Aneurysms.
METHODS
From August 2007 through May 2012, eleven A1 aneurysms in eleven patients were treated endovascularly. Six aneurysms were unruptured and 5 were ruptured. One patient with an unruptured A1 aneurysm presented with subarachnoid hemorrhage due to rupture of an anterior communicating artery aneurysm. Procedural data, clinical and angiographic results were reviewed retrospectively.
RESULTS
All of the aneurysms were successfully treated with coil embolization. Six were treated with a simple technique while the remaining 5 required adjunctive technique : double catheters (n=2), balloon-assisted (n=2), and stent-assisted (n=1). The immediate angiographic control showed a complete occlusion in all cases. Procedure-related complication occurred in only one patient : parent artery occlusion, which was not clinically significant. All patients had excellent clinical outcomes but one patient was discharged with a slight disability. No neurologic deterioration or bleeding was seen during the follow-up period in this cohort of patients. Follow-up angiography (mean, 20 months) was available in ten patients and revealed stable occlusion in all cases.
CONCLUSION
Endovascular treatment is a feasible and effective therapeutic modality for A1 aneurysms. Tailored microcatheter shaping and/or adjunctive techniques are necessary for successful aneurysm embolization because of the projection and location of A1 aneurysms.
MeSH Terms
Figure
-
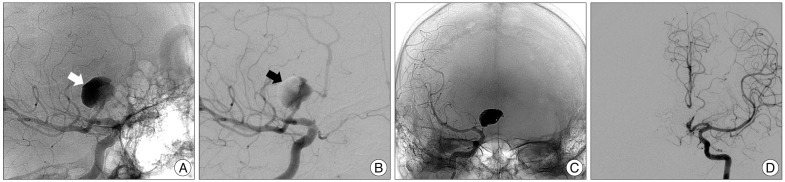
Fig. 1 Patient 10. Images of 42-year-old man with a ruptured large thrombosed aneurysm of right A1. A and B : Unsubtracted and subtracted images of conventional angiography shows a large aneurysm arising from mid-A1. Contrast retention (white arrow) and filling defect (black arrow) in the aneurysm imply a considerable amount of thrombus. C : Unsubtracted images acquired immediately after coiling reveals total occlusion of the aneurysm sac and the ipsilateral A1. D : Left internal carotid angiogram demonstrates sufficient flow of the right anterior cerebral artery provided through the anterior communicating artery.
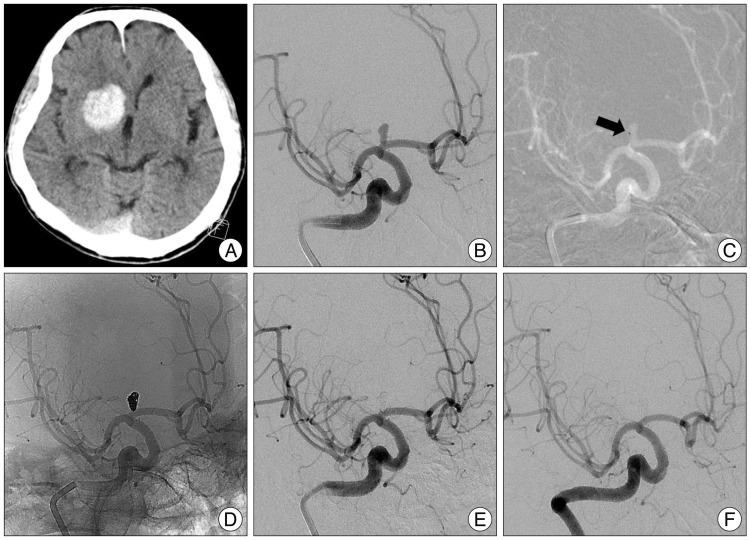
Fig. 2 Patient 11. Images showing a ruptured aneurysm of right A1. A : Computed tomographic examination from a 77-year old male patient with acute ganglionic hemorrhage. B : Conventional angiography shows a right small A1 aneurysm with a small neck. The aneurysm is superiorly located on the parent artery, just a few millimeters after the internal carotid artery bifurcation. C : Roadmap image shows that accurate aneurysm selection with S-shaped microcatheter (arrow) is done and guiding catheter is placed in petrous ICA as distal as possible. D and E : Unsubtracted and subtracted images acquired immediately after coiling reveal complete occlusion of aneurysm. F : The 6 month follow-up angiogram reveals stable occlusion of the aneurysm.
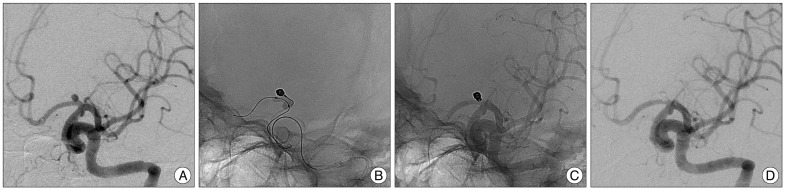
Fig. 3 Patient 1. Images of 47-year-old woman with an unruptured aneurysm of left A1. A : Diagnostic angiography demonstrates a posteriorly projecting saccular aneurysm arising at left proximal A1. Catheterization of aneurysm sac was achieved using a steam-shaped microcatheter in an "S-shape", but compact packing of the aneurysm was not possible due to early kick-back of the microcatheter. B : HyperForm balloon is positioned across the aneurysm neck to stabilize the microcatheter. And the first coil is inserted into the aneurysm with the balloon inflation and bridging the aneurysmal neck. C and D : Unsubtracted and subtracted images acquired immediately after coiling demonstrate dense, complete occlusion of the aneurysm without compromising the parent artery.
Reference
-
1. Barry DM. Surgical treatment of anterior cerebral-anterior communicating artery aneurysms. R I Med J. 1972; 55:245–247. PMID: 4506289.2. Chalif DJ, Weinberg JS. Surgical treatment of aneurysms of the anterior cerebral artery. Neurosurg Clin N Am. 1998; 9:797–821. PMID: 9738108.
Article3. Chang HW, Youn SW, Jung C, Kang HS, Sohn CH, Kwon BJ, et al. Technical strategy in endovascular treatment of proximal anterior cerebral artery aneurysms. Acta Neurochir (Wien). 2011; 153:279–285. PMID: 20872259.
Article4. Czepko R, Libionka W, Lopatka P. Characteristics and surgery of aneurysms of the proximal (A1) segment of the anterior cerebral artery. J Neurosurg Sci. 2005; 49:85–95. PMID: 16288191.5. Dashti R, Hernesniemi J, Lehto H, Niemelä M, Lehecka M, Rinne J, et al. Microneurosurgical management of proximal anterior cerebral artery aneurysms. Surg Neurol. 2007; 68:366–377. PMID: 17905060.
Article6. Gupta R, Horowitz MB, Gilman S. Neuroform stent-assisted coil embolization of a ruptured A1 segment anterior cerebral artery aneurysm. J Neuroimaging. 2006; 16:117–119. PMID: 16629732.
Article7. Handa J, Nakasu Y, Matsuda M, Kyoshima K. Aneurysms of the proximal anterior cerebral artery. Surg Neurol. 1984; 22:486–490. PMID: 6495158.
Article8. Hino A, Fujimoto M, Iwamoto Y, Oka H, Echigo T. Surgery of proximal anterior cerebral artery aneurysms. Acta Neurochir (Wien). 2002; 144:1291–1296. discussion 1296. PMID: 12478340.9. Kassell NF, Torner JC. Size of intracranial aneurysms. Neurosurgery. 1983; 12:291–297. PMID: 6843800.
Article10. Lee HY, Ahn JS, Suh DC, Lee DH. Z-shaped microcatheter tip shaping for embolization of aneurysms at the proximal A1 segment of the anterior cerebral artery : a technical note. Neurointervention. 2011; 6:95–99. PMID: 22125756.
Article11. Lee JM, Joo SP, Kim TS, Go EJ, Choi HY, Seo BR. Surgical management of anterior cerebral artery aneurysms of the proximal (A1) segment. World Neurosurg. 2010; 74:478–482. PMID: 21492598.
Article12. Lubicz B, Bruneau M, Dewindt A, Lefranc F, Balériaux D, De Witte O. Endovascular treatment of proximal anterior cerebral artery aneurysms. Neuroradiology. 2009; 51:99–102. PMID: 18985332.
Article13. Rosner SS, Rhoton AL Jr, Ono M, Barry M. Microsurgical anatomy of the anterior perforating arteries. J Neurosurg. 1984; 61:468–485. PMID: 6747683.
Article14. Serizawa T, Saeki N, Fukuda K, Yamaura A. [Microsurgical anatomy of the anterior communicating artery and its perforating arteries important for interhemispheric trans-lamina terminalis approach : analysis based on cadaver brains]. No Shinkei Geka. 1994; 22:447–454. PMID: 8196831.15. Suzuki M, Onuma T, Sakurai Y, Mizoi K, Ogawa A, Yoshimoto T. Aneurysms arising from the proximal (A1) segment of the anterior cerebral artery. A study of 38 cases. J Neurosurg. 1992; 76:455–458. PMID: 1738027.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Aneurysms of the Proximal Anterior Cerebral Artery
- Ruptured Aneurysm Arising from a Fenestrated A1 Segment of the Anterior Cerebral Artery
- Ruptured Saccular Aneurysm Arising from Fenestrated Proximal Anterior Cerebral Artery : Case Report and Literature Review
- Wire perforation of the missed tiny aneurysm originating from the fenestrated A1 segment during the endovascular approach
- Aneurysms of Proximal(A1) Segment of Anterior Cerebral Artery
