Clinical Analysis of Blepharospasm and Apraxia of Eyelid Opening in Patients with Parkinsonism
- Affiliations
-
- 1Department of Neurology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. wylee@smc.samsung.co
- KMID: 1808486
- DOI: http://doi.org/10.3988/jcn.2005.1.2.159
Abstract
- BACKGROUND AND PURPOSE
Blepharospasm (BSP) and apraxia of eyelid opening (AEO) have been reported as dystonia related with parkinsonism. However, systematic analysis of clinical characteristics of BSP and AEO in parkinsonism has been seldom reported. To investigate the clinical characteristics of BSP and AEO in parkinsonism and to find out the clinical significance to differentiate parkinsonism.
METHODS
We enrolled 35 patients who had BSP with or without AEO out of 1113 patients with parkinsonism (913 IPD, idiopathic Parkinson's disease; 190 MSA, multiple system atrophy, 134 MSA-p, 56 MSA-c and 10 PSP, progressive supranuclear palsy). We subdivided MSA into MSA-p (predominantly parkinsonism) and MSA-c (predominantly cerebellar) according to the diagnostic criteria proposed by Quinn. We analyzed the clinical features of BSP and parkinsonism including onset age, onset interval to BSP, characteristics of BSP, presence of AEO, coexisted dystonias on the other body parts, severity of parkinsonism and relationship with levodopa treatment.
RESULTS
BSP with or without AEO were more frequently observed in atypical parkinsonism (PSP, 70%; MSA-p, 11.2%; MSA-c, 8.9%) than in IPD (0.9%). Reflex BSP was observed only in atypical parkinsonism (4 MSA-p, 1 MSA-c and 2 PSP). BSP preceding parkinsonism (Pre-BSP) was observed mainly in atypical parkinsonism (2 MSA-p, 1 MSA-c, 1 PSP and 1 IPD). The presence of AEO was more frequent in atypical parkinsonism than in IPD, but isolated AEO was not detected. BSP related to levodopa ('off' symptom or 'peak-dose' effect) were observed only in IPD.
CONCLUSIONS
Reflex BSP, Pre-BSP and the presence of AEO may be a unique feature of atypical parkinsonism. BSP related to levodopa might be representative of IPD. No differences were found in the clinical features of BSP between MSA-p and MSA-c.
MeSH Terms
Figure
-
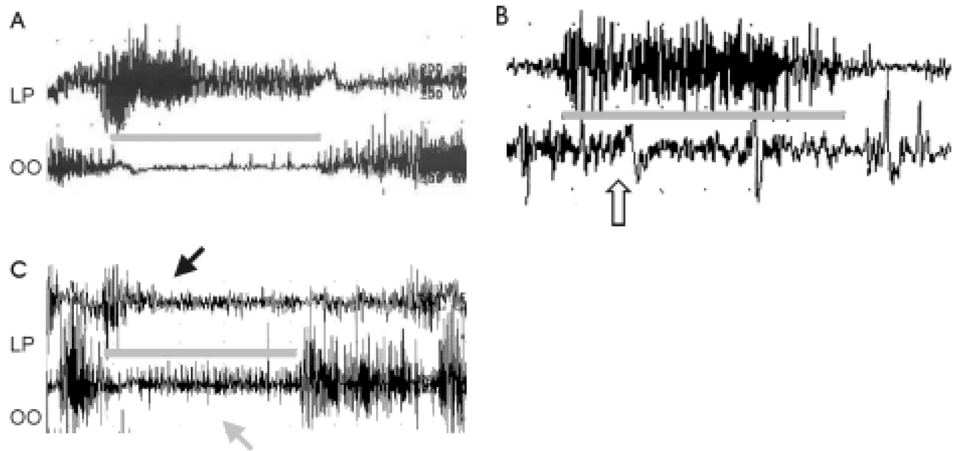
Figure 1 EMG of the levator palpebrae (LP) and orbicularis oculi (OO) in the normal individual (A), in the MSA-p patient with blepharospasm (B) and in the patient with blepharospasm and apraxia of eyelid opening (C). Comparing with normal finding (A), EMG showed a marked contraction of OO (white arrow) during eye opening (gray line) (B). During eye opening, OO inhibition was incomplete (gray arrow) and LP contraction was not sustained (black arrow) (C).
Cited by 1 articles
-
Clinical Perspectives of Parkinson's Disease for Ophthalmologists, Otorhinolaryngologists, Cardiologists, Dentists, Gastroenterologists, Urologists, Physiatrists, and Psychiatrists
Ji-Hyun Choi, Jong-Min Kim, Hee Kyung Yang, Hyo-Jung Lee, Cheol Min Shin, Seong Jin Jeong, Won-Seok Kim, Ji Won Han, In-Young Yoon, Yoo Sung Song, Yun Jung Bae
J Korean Med Sci. 2020;35(28):e230. doi: 10.3346/jkms.2020.35.e230.
Reference
-
1. Grandas F, Elston J, Quinn N, Marsden CD. Blepharospasm: a review of 264 patients. J Neurol Neurosurg Psychiatry. 1988. 51:767–772.
Article2. Hallett M. Blepharospasm: recent advances. Neurology. 2002. 59:1306–1312.
Article3. Jankovic J, Havins WE, Wilkins RB. Blinking and blepharospasm. Mechanism, diagnosis, and management. JAMA. 1982. 248:3160–3164.
Article4. Boghen D. Apraxia of lid opening: a review. Neurology. 1997. 48:1491–1494.5. Lamberti P, De Mari M, Zenzola A, Aniello MS, Defazio G. Frequency of apraxia of eyelid opening in the general population and in patients with extrapyramidal disorders. Neurol Sci. 2002. 23:Suppl 2. S81–S82.
Article6. Lepore FE, Duvoisin RC. "Apraxia" of eyelid opening: an involuntary levator inhibition. Neurology. 1985. 35:423–427.
Article7. Obeso JA, Artieda J, Marsden CD. Stretch reflex blepharospasm. Neurology. 1985. 35:1378–1380.
Article8. Verghese J, Milling C, Rosenbaum DM. Ptosis, blepharospasm, and apraxia of eyelid opening secondary to putaminal hemorrhage. Neurology. 1999. 53:652.
Article9. Miranda M, Millar A. Blepharospasm associated with bilateral infarcts confined to the thalamus: case report. Mov Disord. 1998. 13:616–617.
Article10. Singer C, Schatz NJ, Bowen B, Eidelberg D, Kazumata K, Sternau L, et al. Asymmetric predominantly ipsilateral blepharospasm and contralateral parkinsonism in an elderly patient with a right mesencephalic cyst. Mov Disord. 1998. 13:135–139.
Article11. Kagohashi M, Okuma Y, Fujishima K, Kitada T, Mizuno Y. Blepharospasm associated with multiple system atrophy: a case report and review of the literature. Parkinsonism Relat Disord. 2004. 10:169–171.
Article12. Biousse V, Skibell BC, Watts RL, Loupe DN, Drews-Botsch C, Newman NJ. Ophthalmologic features of Parkinson's disease. Neurology. 2004. 62:177–180.
Article13. Golbe LI, Davis PH, Lepore FE. Eyelid movement abnormalities in progressive supranuclear palsy. Mov Disord. 1989. 4:297–302.
Article14. Dehaene I. Apraxia of eyelid opening in progressive supranuclear palsy. Ann Neurol. 1984. 15:115–116.
Article15. Brusa A, Mancardi G, Meneghini S, Piccardo A, Brusa G. Apraxia' of eye opening in idiopathic Parkinson's disease. Neurology. 1986. 36:134.
Article16. Barclay CL, Lang AE. Dystonia in progressive supranuclear palsy. J Neurol Neurosurg Psychiatry. 1997. 62:352–356.
Article17. Quinn N. Marsden CD, Fahn S, editors. Multiple system atrophy. Movement disorder. 1994. Vol. 3. Oxford: Butterworth-Heinemann;262–281.18. Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. Arch Neurol. 1999. 56:33–39.
Article19. Gilman S, Low PA, Quinn N, Albanese A, Ben-Shlomo Y, Fowler CJ, et al. Consensus statement on the diagnosis of multiple system atrophy. J Neurol Sci. 1999. 163:94–98.
Article20. Litvan I, Agid Y, Calne D, Campbell G, Dubois B, Duvoisin RC, et al. Clinical research criteria for the diagnosis of progressive supranuclear palsy (Steele-Richardson-Olszewski syndrome): report of the NINDS-SPSP international workshop. Neurology. 1996. 47:1–9.
Article21. Jankovic J, Tintner R. Dystonia and parkinsonism. Parkinsonism Relat Disord. 2001. 8:109–121.
Article22. Boesch SM, Wenning GK, Ransmayr G, Poewe W. Dystonia in multiple system atrophy. J Neurol Neurosurg Psychiatry. 2002. 72:300–303.
Article23. Esteban A, Traba A, Prieto J. Eyelid movements in health and disease. The supranuclear impairment of the palpebral motility. Neurophysiol Clin. 2004. 34:3–15.
Article24. Soonawala N, Bhatia KP, Yeung JH, Quinn NP, Marsden CD. Idiopathic blepharospasm does not lead to a parkinsonian syndrome: results of a questionnaire-based follow-up study. J Neurol. 1999. 246:283–286.
Article25. Janati A, Metzer WS, Archer RL, Nickols J, Raval J. Blepharospasm associated with olivopontocerebellar atrophy. J Clin Neuroophthalmol. 1989. 9:281–284.26. Jankovic J, Schwartz KS. Longitudinal experience with botulinum toxin injections for treatment of blepharospasm and cervical dystonia. Neurology. 1993. 43:834–836.
Article27. Poewe WH, Lees AJ, Stern GM. Dystonia in Parkinson's disease: clinical and pharmacological features. Ann Neurol. 1988. 23:73–78.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Apraxia of Eyelid Opening Secondary to Right Thalamic Infarction
- Clinical and EMG Characteristics of Pretarsal Motor Persistence
- Comparison of Clinical and EMG Diagnosis of Involuntary Eyelid Closure
- Apraxia of Eyelid Closing and Unilateral Meige's Syndrome Complicating Left Middle Cerebral Artery Infarction
- Frontalis Suspension Surgery for Patients with Essential Blepharospasm Unresponsive to Botulinum Toxin Injections
