Yonsei Med J.
2010 Jul;51(4):585-589. 10.3349/ymj.2010.51.4.585.
Remifentanil Attenuates Muscle Fasciculations by Succinylcholine
- Affiliations
-
- 1Department of Anaesthesiology and Pain Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
- 2Department of Anaesthesiology and Pain Medicine, Chungnam National University College of Medicine, Daejeon, Korea. yhkim0404@cnu.ac.kr
- 3Department of Rehabilitation Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
- 4Department of Neurology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 5Department of Information Statistics, Chungnam National University, Daejeon, Korea.
- KMID: 1805199
- DOI: http://doi.org/10.3349/ymj.2010.51.4.585
Abstract
- PURPOSE
The present visual and electromyographic study was designed to evaluate muscle fasciculations caused by succinylcholine in adults pretreated with either remifentanil 1.5 microgram/kg or saline.
MATERIALS AND METHODS
The effect of remifentanil on succinylcholine-induced muscle fasciculations was studied using a double-blind method in 40 adults. After i.v. pretreatment with either remifentanil 1.5 microgram/kg (remifentanil group, n = 20) or an equivalent volume of i.v. saline (saline group, n = 20), patients were anaesthetized with a 2.0 mg/kg of i.v. propofol followed by i.v. succinylcholine 1.0 mg/kg. Intensity and duration of muscle fasciculation following i.v. succinylcholine administration were recorded. Electromyography (EMG) was used to quantify the extent of muscle fasciculation following i.v. succinylcholine injection. Myalgia was evaluated 24 hours after induction time. Serum potassium levels were measured five minutes after i.v. succinylcholine administration and creatine kinase (CK) levels 24 hours after induction time.
RESULTS
Compared to saline treated controls, remifentanil decreased the intensity of muscle fasciculations caused by i.v. succinylcholine [fasciculation severity scores (grade 0 to 3) were 2/1/12/5 and 3/13/4/0 (patients numbers) in the saline group and the remifentanil group, respectively, p < 0.001]. The mean (SD) maximum amplitude of muscle action potential (MAP) by EMG was smaller in the remifentanil group [283.0 (74.4) microV] than in the saline group [1480.4 (161.3) microV] (p = 0.003). Postoperative serum CK levels were lower in the remifentanil group (p < 0.001). Postoperative myalgia was not different between the two groups.
CONCLUSION
Remifentanil 1.5 microgram/kg attenuated intensity of muscle fasciculations by succinylcholine.
Keyword
Figure
-
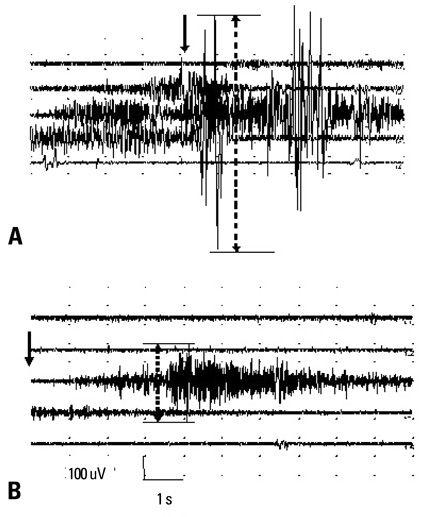
Fig. 1 Typical EMG recordings from the biceps of two patients pretreated with saline or remifentanil. EMG recordings during succinylcholine-induced muscle fasciculation in a patient pretreated with saline (A) or remifentanil (B). Arrows indicate times of i.v. succinylcholine (1.0 mg/kg) administration. Dotted arrow = maximum amplitude. EMG, electromyography.
Reference
-
1. Morris J, Cook TM. Rapid sequence induction: a national survey of practice. Anaesthesia. 2001. 56:1090–1097.
Article2. Mallon WK, Keim SM, Shoenberger JM, Walls RM. Rocuronium vs. succinylcholine in the emergency department: a critical appraisal. J Emerg Med. 2009. 37:183–188.
Article3. Shoroghi M, Zahedi H, Farahbakhsh F, Sheikhvatan M, Abbasi A. The effect of thiopentone on severity and duration of succinylcholine-induced fasciculation. Clin Neuropharmacol. 2009. 32:94–96.
Article4. Kararmaz A, Kaya S, Turhanoglu S, Ozyilmaz MA. Effects of high-dose propofol on succinylcholine-induced fasciculations and myalgia. Acta Anaesthesiol Scand. 2003. 47:180–184.
Article5. Schreiber JU, Lysakowski C, Fuchs-Buder T, Tramèr MR. Prevention of succinylcholine-induced fasciculation and myalgia: a meta-analysis of randomized trials. Anesthesiology. 2005. 103:877–884.6. Brodsky JB, Ehrenwerth J. Postoperative muscle pains and suxamethonium. Br J Anaesth. 1980. 52:215–218.
Article7. Wig J, Bali IM. Relation of precurarization to suxamethonium to provide ease of intubation and to prevent post-suxamethonium muscle pains. Can Anaesth Soc J. 1979. 26:94–98.
Article8. Tsui BC, Reid S, Gupta S, Kearney R, Mayson T, Finucane B. A rapid precurarization technique using rocuronium. Can J Anaesth. 1998. 45:397–401.9. Lindgren L, Saarnivaara L. Effect of competitive myoneural blockade and fentanyl on muscle fasciculation caused by suxamethonium in children. Br J Anaesth. 1983. 55:747–751.
Article10. Yli-Hankala A, Randell T, Varpula T, Lindgren L. Alfentanil inhibits muscle fasciculations caused by suxamethonium in children and in young adults. Acta Anaesthesiol Scand. 1992. 36:588–591.
Article11. Mingus ML, Herlich A, Eisenkraft JB. Attenuation of suxamethonium myalgias. Effect of midazolam and vecuronium. Anaesthesia. 1990. 45:834–837.
Article12. Thompson JP, Hall AP, Russell J, Cagney B, Rowbotham DJ. Effect of remifentanil on the haemodynamic response to orotracheal intubation. Br J Anaesth. 1998. 80:467–469.13. Harvey SC, Roland P, Bailey MK, Tomlin MK, Williams A. At randomized, double-blind comparison of rocuronium, d-tubocurarine, and "mini-dose" succinylcholine for preventing succinylcholine-induced muscle fasciculations. Anesth Analg. 1998. 87:719–722.
Article14. O'Sullivan EP, Williams NE, Calvey TN. Differential effects of neuromuscular blocking agents on suxamethonium-induced fasciculations and myalgia. Br J Anaesth. 1988. 60:367–371.15. Leeson-Payne CG, Nicoll JM, Hobbs GJ. Use of ketorolac in the prevention of suxamethonium myalgia. Br J Anaesth. 1994. 73:788–790.
Article16. Ferres CJ, Mirakhur RK, Criag H, Browne ES, Clarke RS. Pretreatment with vecuronium as a prophylactic against post-suxamethonium muscle pain. Comparison with other non-depolarizing neuromuscular blocking drugs. Br J Anaesth. 1983. 55:735–741.
Article17. Maddineni VR, Mirakhur RK, Cooper AR. Myalgia and biochemical changes following suxamethonium after induction of anaesthesia with thiopentone or propofol. Anaesthesia. 1993. 48:626–628.
Article18. Laurence AS. Myalgia and biochemical changes following intermittent suxamethonium administration. Effects of alcuronium, lignocaine, midazolam and suxamethonium pretreatments on serum myoglobin, creatinine kinase and myalgia. Anaesthesia. 1987. 42:503–510.
Article19. McLoughlin C, Elliott P, McCarthy G, Mirakhur RK. Muscle pains and biochemical changes following suxamethonium administration after six pretreatment regimens. Anaesthesia. 1992. 47:202–206.
Article20. Frederickson RC, Pinsky C. Morphine impairs acetylcholine release but facilitates acetylcholine action at a skeletal neuromuscular junction. Nat New Biol. 1971. 231:93–94.
Article21. Pinsky C, Frederickson RC. Morphine and nalorphine impair neuromuscular transmission. Nat New Biol. 1971. 231:94–96.
Article22. Duke PC, Johns CH, Pinsky C, Goertzen P. The effect of morphine on human neuromuscular transmission. Can Anaesth Soc J. 1979. 26:201–205.
Article23. Cox BM, Weinstock M. The effect of analgesic drugs on the release of acetylcholine from electrically stimulated guinea-pig ileum. Br J Pharmacol Chemother. 1966. 27:81–92.
Article24. Bruce DL, Downs JB, Kulkarni PS, Caplan LM. Precurarization inhibits maximal ventilatory effort. Anesthesiology. 1984. 61:618–621.
Article25. Eisenkraft JB, Mingus ML, Herlich A, Book WJ, Kopman AF. A defasciculating dose of d-tubocurarine causes resistance to succinylcholine. Can J Anaesth. 1990. 37:538–542.
Article26. Rosow C. Remifentanil: a unique opioid analgesic. Ansethesiology. 1993. 79:875–876.27. Miller RD, Way WL. Inhibition of succinylcholine-induced increased intragastric pressure by nondepolarizing muscle relaxants and lidocaine. Anesthesiology. 1971. 34:185–188.
Article28. Barclay K, Kluger MT. Effect of bolus dose of remifentanil on haemodynamic response to tracheal intubation. Anaesth Intensive Care. 2000. 28:403–407.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- What`s the optimal timing of pretreatment with pancuronium before succinylcholine to prevent muscle fasciculation?
- Rocuronium and Lidocaine Pretreatment for Prevention of Biochemical Changes, Fasciculations and Myalgia following Succinylcholine Administration
- Precurarization Effects of the Interval between Pretreatment with Rocuronium or Vecuronium and Succinylcholine Administration
- Rocuronium Pretreatment for Prevention of Myalgia Following Succinylcholine Administration
- Optimal Priming Dose of Rocuronium for Prevention of Succinylcholine Induced Fasciculations
