Posterior triangle approach for lateral in-plane technique during hemodialysis catheter insertion via the internal jugular vein
- Affiliations
-
- 1Department of Surgery, Soonchunhyang University College of Medicine, Seoul, Korea. ultravascsurg@gmail.com
- KMID: 1804130
- DOI: http://doi.org/10.4174/astr.2015.88.2.114
Abstract
- A recent widespread concept is that ultrasound-guided central venous catheter insertion is a mandatory method. Some techniques have been introduced for ultrasound-guided central venous catheterization. Among them, short-axis lateral in-plane technique is considered to be the most useful technique for internal jugular vein access. Therefore, we used this technique for the insertion of a large-bore cuffed tunneled dual-lumen catheter for hemodialysis. Additionally, a lesser number of catheter angulations may lead to good flow rates and catheter function; we recommend that skin puncture site in the neck at the posterior triangle is better than the Sedillot's triangle. Using this approach, we can reduce the possible complications of pinching and kinking of the catheter.
MeSH Terms
Figure
-

Fig. 1 (A) Ultrasound-guided needle puncture image using the short axis lateral in-plane technique; Image shows the puncture needle, internal jugular vein (IJV), carotid artery (CA), and the sternocleidomastoid (SCM) muscle. The tip of the needle inside the IJV along with the entire course of the needle is identified. The needle is passed from the posterior triangle, through the nonmuscular area under the SCM muscle. The course of the needle is angled at about 30° to a horizontal line. (B) CT image using the short axis lateral in-plane technique. Needle drives a horizontal line from the posterior triangle. The trajectory of the needle from the Sedillot's triangle forms an angle of about 30°-45° against the horizontal line. (C) The course of needle from Sedillot's triangle has two mixed curvatures; rotation and downward. (D) The immediate C-arm fluoroscope image confirmed that the catheter was not kinking. The catheter's midline was kept in the middle of the catheter throughout the full length.
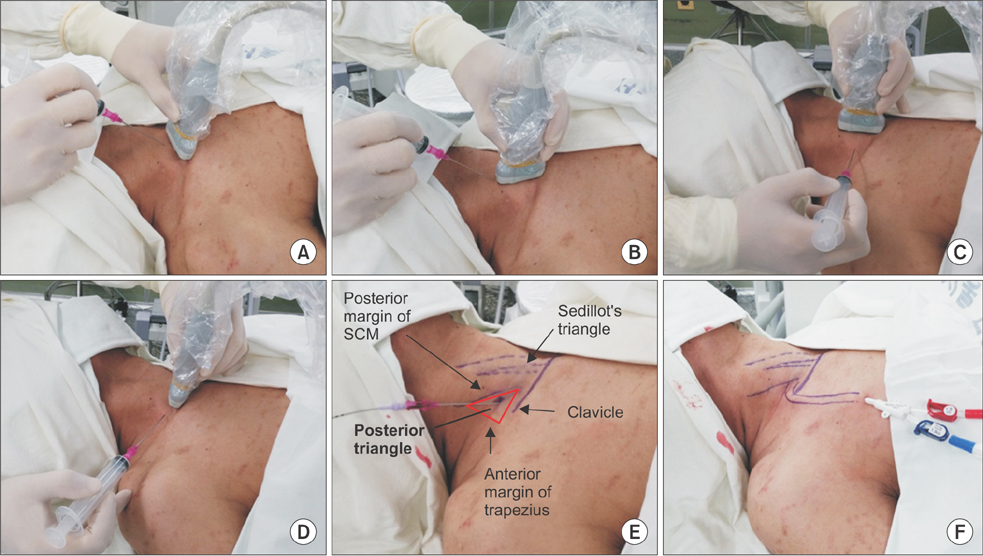
Fig. 2 (A) Short axis, Out-of-Plane (Vertical) approach. (B) Long axis, in-plane approach. (C) Long axis, lateral out-of-plane approach. (D) Short axis, lateral in-plane technique; it allows simultaneous view of the full length of the needle, the internal jugular vein, carotid artery, and adjacent tissue. (E) Puncture needle was inserted at the posterior triangle, which consisted of posterior margin of the sternocleidomastoid muscle, anterior margin of the trapezius muscle, and clavicle. (F) A completely inserted catheter had a smooth curvature over the clavicle while maintaining its horizontal line, and did not show any kinking.
Reference
-
1. Cho JB, Park IY, Sung KY, Baek JM, Lee JH, Lee DS. Pinch-off syndrome. J Korean Surg Soc. 2013; 85:139–144.2. Bannon MP, Heller SF, Rivera M. Anatomic considerations for central venous cannulation. Risk Manag Healthc Policy. 2011; 4:27–39.3. Lamperti M, Bodenham AR, Pittiruti M, Blaivas M, Augoustides JG, Elbarbary M, et al. International evidence-based recommendations on ultrasound-guided vascular access. Intensive Care Med. 2012; 38:1105–1117.4. Hind D, Calvert N, McWilliams R, Davidson A, Paisley S, Beverley C, et al. Ultrasonic locating devices for central venous cannulation: meta-analysis. BMJ. 2003; 327:361.5. Rossi UG, Rigamonti P, Ticha V, Zoffoli E, Giordano A, Gallieni M, et al. Percutaneous ultrasound-guided central venous catheters: the lateral in-plane technique for internal jugular vein access. J Vasc Access. 2014; 15:56–60.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- ERRATUM: Correction of affiliation: Posterior triangle approach for lateral in-plane technique during hemodialysis catheter insertion via the internal jugular vein
- Cut-down method for perm catheter insertion in patients with completely occluded internal jugular vein
- Right Internal Jugular Venous Thrombosis Occurred after Long-term Placement of Hemodialysis Catheter Inserted Via Right Subclavian Vein: A Case Report
- A case of paroxysmal atrial fibrillation induced by internal jugular venous catheterization for hemodialysis
- The difference of complications and overall survival according to the types of vascular access in hemodialysis
