Osteochondral Lesion of the Bilateral Femoral Heads in a Young Athletic Patient
- Affiliations
-
- 1Department of Radiology, Kyung Hee University Hospital, Seoul 130-872, Korea. t2star@naver.com
- 2Department of Orthopedic Surgery, Kyung Hee University Hospital, Seoul 130-872, Korea.
- 3Department of Radiology, Kyung Hee University Hospital at Gangdong, Kyung Hee University College of Medicine, Seoul 134-727, Korea.
- 4Department of Radiology, Jeju National University Hospital, Jeju 690-767, Korea.
- KMID: 1794651
- DOI: http://doi.org/10.3348/kjr.2014.15.6.792
Abstract
- Osteochondral lesions of the femoral head are uncommon and few studies have reported their imaging findings. Since joints are at risk of early degeneration after osteochondral damage, timely recognition is important. Osteochondral lesions of femoral head may often be necessary to differentiate from avascular necrosis. Here, we report a case of osteochondral lesions on bilateral femoral heads. This lesion manifested as subchondral cysts in initial radiographs, which led to further evaluation by computed tomography arthrography and magnetic resonance imaging, which revealed overlying cartilage defects.
Keyword
MeSH Terms
Figure
-
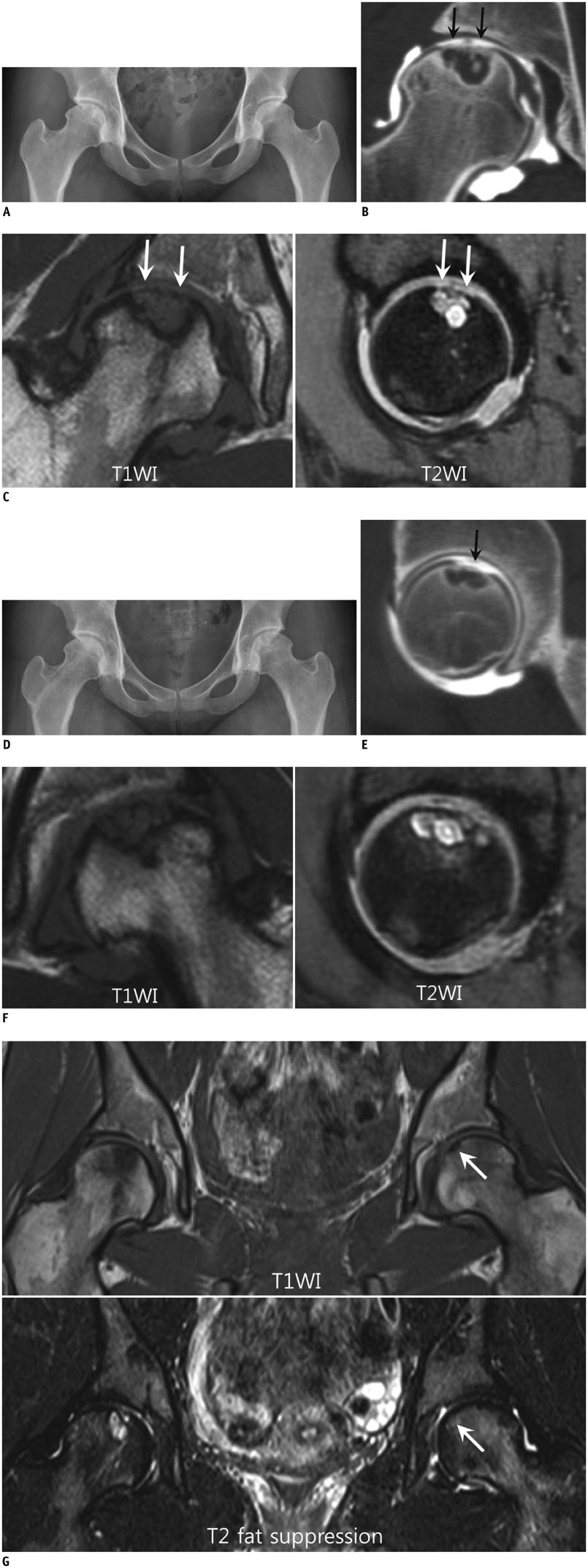
Fig. 1 Osteochondral lesions of bilateral femoral heads in 20-year-old female. A. Plain radiography image of right hip shows several subchondral cysts in superior portion of femoral head. Left femoral head shows no remarkable finding. B. Coronal CT arthrography image of right hip show several subchondral cysts with overlying articular cartilage defects and fissuring (arrows) in superior portion of right femoral head. C. Lesion shows hypointensity on coronal T1-weighted MRI (TR/TE, 374/20) (T1WI) (arrows) and hyperintensity on sagittal T2-weighted MRI (TR/TE, 1500/29) (T2WI) (arrows) that were immediately obtained after CT arthrography. Overlying articular cartilage defects and fissuring are noted. No evidence of bone marrow edema of femoral head is present. D. One year after surgery on right hip, plain radiography of left hip demonstrates several subchondral cysts in superior portion of left femoral head. Surgical bone change of core decompression with bone graft is noted on right femur. E. Sagittal CT arthrography image of left hip show newly developed several subchondral cysts with overlying cartilage defects and fissuring (arrow) in superior portion of left femoral head. TE = echo time, TR = repetition time. F. Coronal T1-weighted MRI (TR/TE, 374/20) (T1WI) and sagittal T2-weighted MRI (TR/TE, 1500/29) (T2WI) show similar lesion, which manifested in right femoral head. G. MRI of local referral hospital obtained 2 months before first visit to our hospital. Coronal T1WI (TR/TE, 666/12) shows wedge shaped area of hypointensity in superomedial portion of left femoral head (arrow). Coronal T2WI with fat suppression (TR/TE, 4460/57) shows corresponding area of hyperintensity (arrow). Overlying articular cartilage is difficult to observe on these images. Subchondral cysts are seen in right femoral head. TE = echo time, TR = repetition time
Reference
-
1. Bohndorf K. Imaging of acute injuries of the articular surfaces (chondral, osteochondral and subchondral fractures). Skeletal Radiol. 1999; 28:545–560.2. Felson DT. Clinical practice. Osteoarthritis of the knee. N Engl J Med. 2006; 354:841–848.3. Edmonds EW, Heyworth BE. Osteochondritis dissecans of the shoulder and hip. Clin Sports Med. 2014; 33:285–294.4. Visuri T. Stress osteopathy of the femoral head. 10 military recruits followed for 5-11 years. Acta Orthop Scand. 1997; 68:138–141.5. Lindén B, Jonsson K, Redlund-Johnell I. Osteochondritis dissecans of the hip. Acta Radiol. 2003; 44:67–71.6. Nakamura Y, Mitsui H, Toh S, Echigoya N. Osteochondral lesion of the femoral head in a fencer: a case report. Am J Orthop (Belle Mead NJ). 2009; 38:356–359.7. Kusumi T, Ishibashi Y, Tsuda E, Kusumi A, Tanaka M, Sato F, et al. Osteochondritis dissecans of the elbow: histopathological assessment of the articular cartilage and subchondral bone with emphasis on their damage and repair. Pathol Int. 2006; 56:604–612.8. Linden B. Osteochondritis dissecans of the femoral condyles: a long-term follow-up study. J Bone Joint Surg Am. 1977; 59:769–776.9. Osterman K, Lindholm TS. Osteochondritis dissecans following Perthes' disease. Clin Orthop Relat Res. 1980; (152):247–254.10. Weaver CJ, Major NM, Garrett WE, Urbaniak JE. Femoral head osteochondral lesions in painful hips of athletes: MR imaging findings. AJR Am J Roentgenol. 2002; 178:973–977.11. Stoller DW. Magnetic resonance imaging in orthopaedics and sports medicine. 3rd ed. Philadelphia: Lippincott Williams & Wilkins;2007. p. 121–134.12. Sakai T, Sugano N, Nishii T, Haraguchi K, Ochi T, Ohzono K. MR findings of necrotic lesions and the extralesional area of osteonecrosis of the femoral head. Skeletal Radiol. 2000; 29:133–141.13. Edwards DJ, Lomas D, Villar RN. Diagnosis of the painful hip by magnetic resonance imaging and arthroscopy. J Bone Joint Surg Br. 1995; 77:374–376.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Femoral Head Fracture with Hip Dislocation Treated by Autologous Osteochondral Transfer (Mosaicplasty) - A Case Report -
- Autologous Osteochondral Transplantation as a Secondary Procedure after Failed Microfracture for Osteochondral Lesion of Talus
- Simultaneously Occurred Medial and Lateral Osteochondral Lesions of the Talus
- Short-Term Results of Osteochondral Autologous Transfer and Femoral Neck Osteochondroplasty for the Treatment of Osteochondral Lesions of the Femoral Head and Concomitant Femoroacetabular Impingement Syndrome: A Case Series
- Bilateral Osteochondritis Dissecans of the Femoral Condyles in Both Knees: A Report of Two Sibling Cases
