J Korean Med Sci.
2009 Feb;24(1):176-178. 10.3346/jkms.2009.24.1.176.
Lupus Myocarditis Presenting as Acute Congestive Heart Failure: A Case Report
- Affiliations
-
- 1Department of Cardiology, School of Medicine, Ajou University, Suwon, Korea. hwanggs@ajou.ac.kr
- KMID: 1794429
- DOI: http://doi.org/10.3346/jkms.2009.24.1.176
Abstract
- A young woman who had a delivery history 3 months previously presented with dyspnea and orthopnea. Initial findings of physical examination, chest radiography, and echocardiogram showed typical congestive heart failure with severe left ventricular (LV) dysfunction. At first, we considered peripartum cardiomyopathy because she had given birth to a baby 3 months previously. However, even though we massively tried conventional drug therapy for 10 days, the patient still remained with refractory heart failure. We performed additional laboratory studies such as complement level and autoantibodies, of which the results supported systemic lupus erythematosus. We could make the diagnosis of acute lupus myocarditis and treated her with corticosteroid. The symptoms were dramatically disappeared and LV function also improved.
MeSH Terms
-
Acute Disease
Administration, Oral
Adult
Echocardiography
Female
Glucocorticoids/administration & dosage
Heart Failure/*diagnosis
Humans
Lupus Erythematosus, Systemic/complications/*diagnosis/radiography
Methylprednisolone/administration & dosage
Myocarditis/*diagnosis/etiology/radiography
Prednisolone/administration & dosage
Figure
-
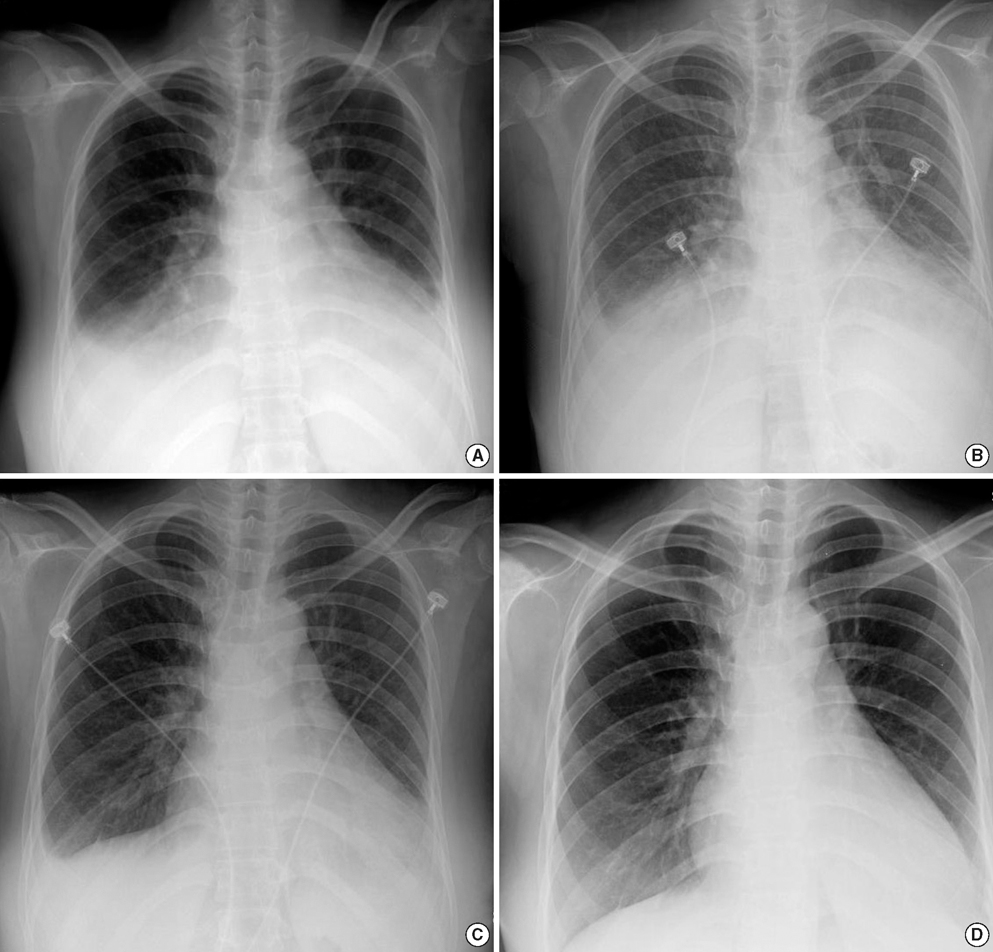
Fig. 1 Chest radiography in time sequence A through D. (A) showed cardiomegaly, interstitial pulmonary edema and pleural effusion on admission. (B) showed interstitial pulmonary edema and pleural effusion were still remained after intensive customary heart failure therapy for 10 days. Pulmonary edema and pleural effusion were dramatically decreased in 48 hr (C) and disappeared in 2 weeks (D) after corticosteroid therapy.

Fig. 2 Two-dimensional echocardiography on admission (A) and 2 weeks after corticosteroid therapy (B). Left ventricular function was much improved with corticosteroid therapy. LVEF, left ventricular ejection fraction; LVEDD, left ventricular end-diastolic dimension; LVESD, left ventricular end-systolic dimension.
Reference
-
1. Wijetunga M, Rockson S. Myocarditis in systemic lupus erythematosus. Am J Med. 2002. 113:419–423.
Article2. Tan EM, Cohen AS, Fries JF, Masi AT, Mcshane DJ, Rothfield NF, Schaller JG, Talal N, Winchester RJ. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982. 25:1271–1277.
Article3. Feldman AM, McNamara D. Myocarditis. N Engl J Med. 2000. 343:1388–1398.
Article4. Kalke S, Balakrishanan C, Mangat G, Mittal G, Kumar N, Joshi VR. Echocardiography in systemic lupus erythematosus. Lupus. 1998. 7:540–544.
Article5. Frustaci A, Gentiloni N, Caldarulo M. Acute myocarditis and left ventricular aneurysm as presentations of systemic lupus erythematosus. Chest. 1996. 109:282–284.
Article6. Naarendorp M, Kerr LD, Khan AS, Ornstein MH. Dramatic improvement of left ventricular function after cytotoxic therapy in lupus patients with acute cardiomyopathy: report of 6 cases. J Rheumatol. 1999. 26:2257–2260.7. Chan YK, Li EK, Tam LS, Chow LT, Ng HK. Intravenous cyclophosphamide improves cardiac dysfunction in lupus myocarditis. Scand J Rheumatol. 2003. 32:306–308.
Article8. Sherer Y, Levy Y, Shoenfeld Y. Marked improvement of severe cardiac dysfunction after one course of intravenous immunoglobulin in a patient with systemic lupus erythematosus. Clin Rheumatol. 1999. 18:238–240.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acute Fulminant Myocarditis Progressed into and Recovered from Congestive Heart Failure and Multiorgan Failure
- Systemic Lupus Erythematosus Presenting as Acute Lupus Myocarditis
- Current Opinion in Viral Myocarditis and Dilated Cardiomyopathy: New Paradigms for Congestive Heart Failure
- A Case of Neonatal Lupus Syndrome with Acute Myocarditis
- A Case of Kawasaki Disease in a 16-year-old Girl Associated with Congestive Heart Failure
