Hepatic Actinomycosis Mimicking a Malignant Tumor: Three Case Reports
- Affiliations
-
- 1Department of Radiology, Yeungnam University College of Medicine, Daegu, Korea. sungho1999@ynu.ac.kr
- KMID: 1793893
- DOI: http://doi.org/10.3348/jksr.2015.72.5.352
Abstract
- Various forms of hepatic actinomycosis can be observed on the imaging studies. We report here the imaging findings of three cases of hepatic actinomycosis, which presented as a solid mass mimicking a malignant tumor. With respect to their enhancement pattern on the contrast-enhanced CT and MR images, one case showed homogeneous and persistent enhancement throughout three phases, while the other two cases showed variable degrees of delayed enhancement with their own features during the portal and equilibrium phases, suggesting that they have abundant fibrosis at different stages. Also, normal vascular structures traversing the masses were noted in all three cases. One core needle biopsy and two surgical resections were performed, and the masses were pathologically proven to be hepatic actinomycosis. In conclusion, we need to be aware that a hepatic tumor with abundant fibrosis, in which the normal vasculature is traversing, can be diagnosed as hepatic actinomycosis.
Figure
-
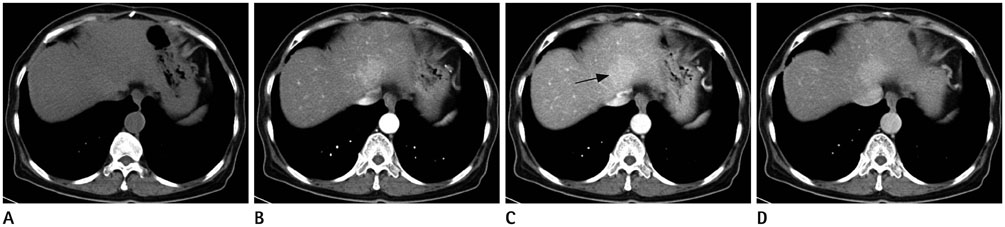
Fig. 1 65-year-old female with hepatic actinomycosis. A. Non-enhanced CT image shows an ill-defined, hypoattenuating mass in the left lobe of the liver. B-D. Contrast-enhanced CT image show the same hyperattenuating mass with homogenous and prolonged enhancement throughout the arterial (B), portal (C), and equilibrium (D) phases, as compared with the liver parenchyma, indicating that the mass is hypervascular, and also has delayed enhancement. Note tiny spots in the mass (arrow), representing normal vascular structures traversing the mass.
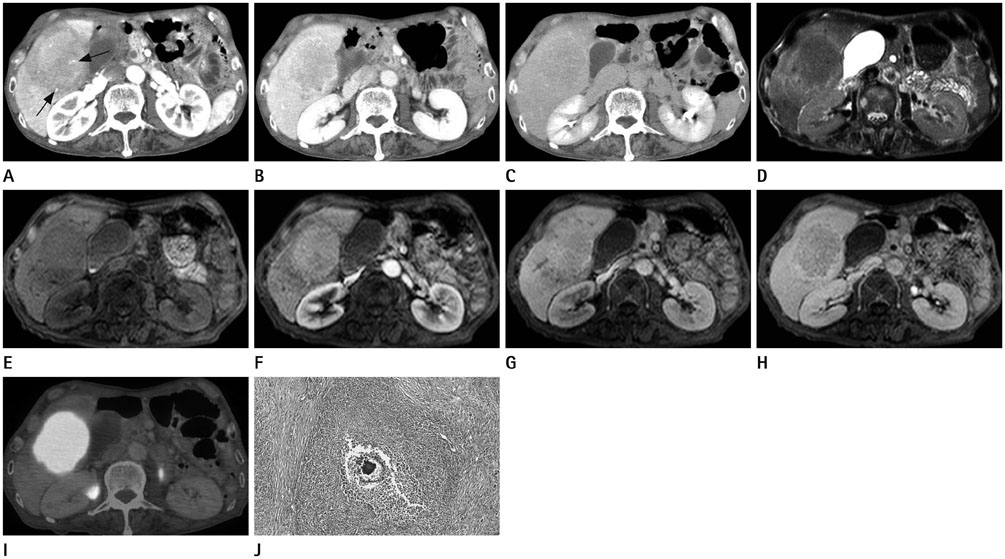
Fig. 2 68-year-old male with hepatic actinomycosis. A. The arterial phase CT image shows an ill-defined, hypoattenuating mass with more hypoattenuating outer layer and less hypoattenuating central portion (i.e., slightly hypervascular), in the right lobe of the liver, as compared with the liver parenchyma. Transient enhancement of the liver parenchyma is seen, probably due to hyperemic inflammatory change. Strongly enhancing, normal vascular structures traversing the mass are seen in the mass (arrows). B. On the portal phase CT image, the outer layer of the mass becomes to be iso-attenuating or slightly hyperattenuating, while its central portion becomes to be hypoattenuating, as compared with the liver parenchyma. C. On the venous phase CT image, the same mass becomes to be almost isoattenuating, as compared with the liver parenchyma, representing delayed enhancement of both outer layer and central portion with different degrees. Delayed-enhancing, internal septa and rim-like layer inside the outer layer are also seen on the portal and venous phases. D. On the T2-weighted magnetic resonance (MR) image, the same mass shows the slightly hyperintense outer layer and almost iso-intense central portion, as compared with the liver parenchyma. E. Non-enhanced T1-weighted MR image shows a hypointense mass with slightly more hypointense outer layer, as compared with the liver parenchyma. F-H. Dynamic contrast-enhanced T1-weighted MR images show the same mass with the slightly hyperintense central portion (i.e., slightly hypervacular) and slightly hypointense outer layer, as compared with the liver parenchyma, on the arterial phase (F), of which the outer layer becomes to be more hyperintense than those of the central portion and liver parenchyma during the portal (G) and venous (H) phase MR images, as shown in the portal phase CT image. I. Positron emission tomography-CT shows the same mass with avid 18F-fluorodeoxyglucose uptake. J. On the hematoxylin and eosin stain (× 40), characteristic sulfur granule of actinomycosis and neutrophils with surrounding fibrous septa are observed.

Fig. 3 27-year-old male with hepatic actinomycosis. A. Arterial phase CT image shows a heterogeneously hypoattenuating mass with more hypoattenuating peripheral rim and internal septa in the left lobe of the liver, as compared with the liver parenchyma. Also seen is hyperemic change of the liver parenchyma around the mass. Strongly enhancing, normal vascular structures are also seen in the mass (arrow). B, C. The peripheral rim and internal septa are gradually and clearly enhancing during the portal (B) and delayed (C) phase CT images, representing delayed enhancement. D. On the T2-weighted magnetic resonance (MR) image, the same mass appears to be slightly hyperintense with heterogeneous signal intensities, as compared with the liver parenchyma. Also noted are normal vascular structures with bright signal intensity traversing the mass. E. Non-enhanced T1-weighted MR image shows the same hypointense mass with heterogeneous signal intensities, as compared with the liver parenchyma. F-H. Dynamic contrast-enhanced T1-weighted MR images show delayed enhancement of peripheral rim and internal septa throughout the arterial (F), portal (G), and venous (H) phase MR images similar to those of CT images. I. Positron emission tomography-CT shows the same mass with avid 18F-fluorodeoxyglucose uptake.
Reference
-
1. Shah HR, Williamson MR, Boyd CM, Balachandran S, Angtuaco TL, McConnell JR. CT findings in abdominal actinomycosis. J Comput Assist Tomogr. 1987; 11:466–469.2. Kim HS, Park NH, Park KA, Kang SB. A case of pelvic actinomycosis with hepatic actinomycotic pseudotumor. Gynecol Obstet Invest. 2007; 64:95–99.3. Kasano Y, Tanimura H, Yamaue H, Hayashido M, Umano Y. Hepatic actinomycosis infiltrating the diaphragm and right lung. Am J Gastroenterol. 1996; 91:2418–2420.4. Lai AT, Lam CM, Ng KK, Yeung C, Ho WL, Poon LT, et al. Hepatic actinomycosis presenting as a liver tumour: case report and literature review. Asian J Surg. 2004; 27:345–347.5. Sharma M, Briski LE, Khatib R. Hepatic actinomycosis: an overview of salient features and outcome of therapy. Scand J Infect Dis. 2002; 34:386–391.6. Miyamoto MI, Fang FC. Pyogenic liver abscess involving Actinomyces: case report and review. Clin Infect Dis. 1993; 16:303–309.7. Ha HK, Lee HJ, Kim H, Ro HJ, Park YH, Cha SJ, et al. Abdominal actinomycosis: CT findings in 10 patients. AJR Am J Roentgenol. 1993; 161:791–794.8. Hochsztein JG, Koenigsberg M, Green DA. US case of the day. Actinomycotic pelvic abscess secondary to an IUD with involvement of the bladder, sigmoid colon, left ureter, liver, and upper abdominal wall. Radiographics. 1996; 16:713–716.9. Ko SW, Jung YY, Kang HK. MR findings of hepatic actinomycosis: case report. J Korean Radiol Soc. 2003; 48:327–330.10. Isozaki T, Numata K, Kiba T, Hara K, Morimoto M, Sakaguchi T, et al. Differential diagnosis of hepatic tumors by using contrast enhancement patterns at US. Radiology. 2003; 229:798–805.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- MR Findings of Hepatic Actinomycosis: Case Report
- Unique Imaging Features in Hepatic Actinomycosis Accompanied by an IgG4-Related Inflammatory Pseudotumor: A Case Report
- Primary Hepatic Actinomycosis Mimicking Hepatic Malignancy with Metastatic Lymph Nodes by F-18 FDG PET/CT
- A case of primary hepatic actinomycosis
- Abdominopelvic Actinomycosis Mimicking Peritoneal Carcinomatosis: A Case Report
