Needle Knife-assisted Endoscopic Polypectomy for a Large Inflammatory Fibroid Colon Polyp by Making Its Stalk into an Omega Shape Using an Endoloop
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. geniushee@yuhs.ac
- 2Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- 3Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1793209
- DOI: http://doi.org/10.3349/ymj.2008.49.4.680
Abstract
- Colonic inflammatory fibroid polyp (IFP) is an uncommon benign polypoid lesion, which is composed of fibroblasts, numerous small vessels and edematous connective tissue with marked eosinophilic inflammatory cell infiltration. This condition is frequently detected in the stomach and small intestine, but uncommon in the colon. Although IFP is a benign lesion, surgical resections are performed in most colonic cases because the polyps are usually too large to resect endoscopically. Only three patients underwent endoscopic polypectomy in our literature reviews. Here, we present a case of IFP in the descending colon successful endoscopically resected using a novel technique of trapping its stalk with an endoloop, forming the stalk into an omega shape, and then dissecting the stalk with a needle knife.
MeSH Terms
Figure
-
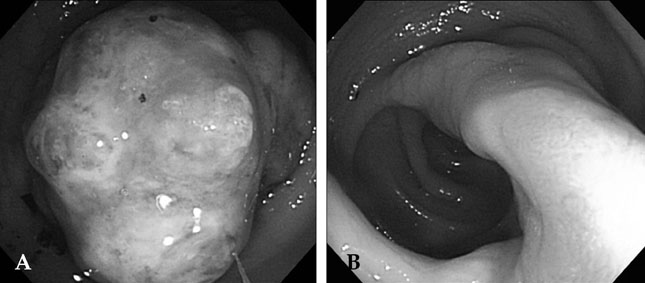
Fig. 1 Colonoscopic findings demonstrated a 4.5 cm-sized pedunculated polyp (A) with multiple surface erosions, exudates, and nodules on its head and long, thick stalk (B) in the distal descending colon. The polyp occupied nearly the entire colonic lumen.

Fig. 2 The polyp was treated by needle knife assisted endoscopic polypectomy because of the difficulty in trapping the large pedunculated shape using an endoloop. For the first step, an endoclip was positioned to partially clamp the stalk (A). Next, hypertonic saline was injected at the base of stalk (B). Dissection of the stalk with a needle knife was attempted, but significant bleeding from the stalk was observed, and consequently dissection was stopped. Next, we tried to trap the polyp with an endoloop, which was not satisfactorily performed due to the large head and rambling mobility of the polyp. Endolooping was finally carried out by tightly seizing the omega shaped stalk (C). We reinserted the scope with a translucent cap, and dissected the stalk of the polyp with a needle knife (D).
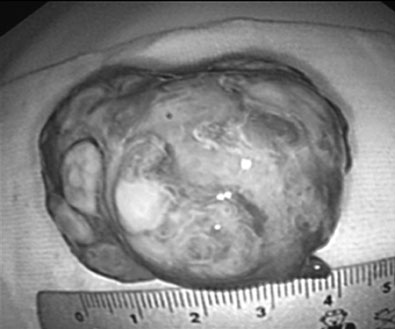
Fig. 3 The specimen was 4.5 × 2.8 × 3.0 cm in size, had multiple nodules, and an erosive surface with exudates.
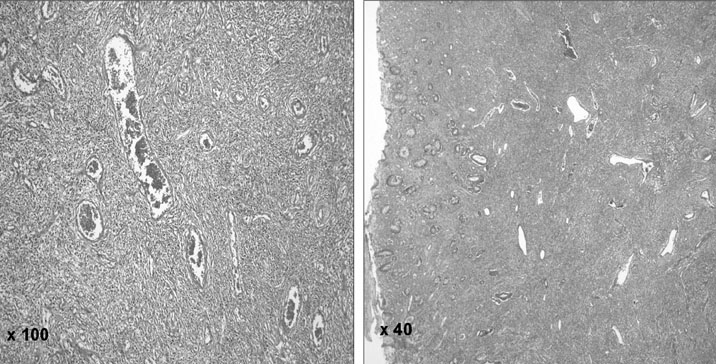
Fig. 4 Microscopic findings showed mucosal ulceration with the proliferation of stromal cells, onion-skin-like spindle-shaped cells, lymphocytes, many vascular structures, fibrosis and eosinophils, which is consistent with an inflammatory fibroid polyp (hematoxylin and eosin stain).

Fig. 5 The illustration of schematic polypectomy procedure in our case. For the first step, the colonoscope approached the stalk of polyp with endoloop slowly expanded (A). Next, we pushed up the stalk with the scope making it crooked and further expanded the endoloop simultaneously (B). Endolooping was finally carried out by tightly seizing the stalk into omega shape (C). The scope with a translucent cap was inserted again, and the proximal portion of stalk was dissected with a needle knife (D).
Reference
-
1. Kim YI, Kim WH. Inflammatory fibroid polyps of gastrointestinal tract. Evolution of histologic patterns. Am J Clin Pathol. 1988. 89:721–727.2. Shimer GR, Helwig EB. Inflammatory fibroid polyp of the intestine. Am J Clin Pathol. 1984. 81:708–714.3. Johnstone JM, Morson BC. Inflammatory fibroid polyp of the gastrointestinal tract. Histopathology. 1978. 10:349–361.4. Hasegawa T, Yang P, Kagawa N, Hirose T, Sano T. CD34 expression by inflammatory fibroid polyps of the stomach. Mod Pathol. 1997. 10:451–456.5. Kim MK, Higgins J, Cho EY, Ko YH, Oh YL. Expression of CD34, bcl-2, and kit in inflammatory fibroid polyps of the gastrointestinal tract. Appl Immunohistochem Mol Morphol. 2000. 8:147–153.
Article6. Stolte M, Finkenzeller G. Inflammatory fibroid polyp of the stomach. Endoscopy. 1990. 22:203–207.7. Merkel IS, Rabinovitz M, Dekker A. Cecal inflammatory fibroid polyp presenting with chronic diarrhea. A case report and review of the literature. Dig Dis Sci. 1992. 37:133–136.8. Gooszen AW, Tjon A, Tham RT, Veselic M, Bolk JH, Lamers CB. Inflammatory fibroid polyp stimulating malignant tumor of the colon in a patient with multiple hamartoma syndrome (Cowden's disease). AJR Am J Roentgenol. 1995. 165:1012–1013.
Article9. de la Plaza R, Picardo AL, Cuberes R, Jara A, Martìnez-Peñalver I, Villanueva MC, et al. Inflammatory fibroid polyps of the large intestine. Dig Dis Sci. 1999. 44:1810–1816.10. Helwig EB, Ranier A. Inflammatory fibroid polyps of the stomach. Surg Gynecol Obstet. 1953. 96:335–367.11. Eslami-Varzaneh F, Washington K, Robert ME, Kashgarian M, Goldblum JR, Jain D. Benign fibroblastic polyps of the colon: a histologic, immunohistochemical, and ultrastructural study. Am J Surg Pathol. 2004. 28:374–378.12. Makhlouf HR, Sobin LH. Inflammatory myofibroblastic tumors (inflammatory pseudotumors) of the gastrointestinal tract: how closely are they related to inflammatory fibroid polyps? Hum Pathol. 2002. 33:307–315.13. Price B. McGee JO, Isaacson PG, Wright NA, Dick HM, Slack MPE, editors. Inflammatory fibroid polyp. Oxford textbook of pathology. 1992. Oxford: Oxford University Press;1249.14. Pardo Menendez V, Rodriguez Tapia I. Eosinophilic granuloma of the colon. Arch Hosp Univ. 1952. 4:248–253.15. Kofler E. Granulomata of the gastrointestinal tract. Virchows Arch. 1952. 321:121–133.16. Vitolo RE, Rachlin SA. Infammatory fibroid polyp of large intestine; report of a case. J Int Coll Surg. 1955. 23:700–709.17. McGee HJ Jr. Infammatory fibroid polyps of the ileum and cecum. Arch Pathol. 1960. 70:203–207.18. Samter TG, Alstott DF, Kurlander GJ. Inflammatory fibroid polyps of the gastrointestinal tract. A report of 3 cases, 2 occurring in children. Am J Clin Pathol. 1966. 45:420–436.
Article19. Zimmerman HG. Eosinophilic granuloma of the ascending colon (author's transl). Z Gastroenterol. 1977. 15:676–679.20. Benjamin SP, Hawk WA, Turnbull RB. Fibrous inflammatory polyps of the ileum and cecum: review of five cases with emphasis on differentiation from mesenchymal neoplasm. Cancer. 1977. 39:1300–1305.21. Lifschitz O, Lew S, Witz M, Reiss R, Griffel B. Inflammatory fibroid polyp of sigmoid colon. Dis Colon Rectum. 1979. 22:575–577.22. Matsuzaki S, Kikuchi K, Iwamura K, Inaba M, Sugimoto E, Itakura M, et al. A case of eosinophilic granuloma (inflammatory fibroid polyp) of the colon (author's transl). Nippon Shokakibyo Gakkai Zasshi. 1979. 76:126–132. (in Japanese).23. Ferin P, Skucas J. Inflammatory fibroid polyp of the colon simulating malignancy. Radiology. 1985. 149:55–56.24. Pollice L, Bufo P. Inflammatory fibroid polyp of the rectum. Pathol Res Pract. 1984. 178:508–512.
Article25. Niv Y, Hurwitz A. Inflammatory fibroid polyp of the cecum, associated with adenomatous polyp and ovarian thecoma. Isr J Med Sci. 1985. 21:624–626.26. Harned RK, Buck JL, Shekitka KM. Inflammatory fibroid polyps of the gastrointestinal tract: radiologic evaluation. Radiology. 1992. 182:863–866.
Article27. Nakase H, Mimura J, Kawasaki T, Itani T, Komori H, Hashimoto K, et al. Endoscopic resection of small inflammatory fibroid polyp of the colon. Intern Med. 2000. 39:25–27.
Article28. Sakamoto T, Kato H, Okabe T, Ohya T, Iesato H, Yokomori T, et al. A large inflammatory fibroid polyp of the colon treated by endoclip-assisted endoscopic polypectomy: A case report. Dig Liver Dis. 2005. 37:968–972.29. Cho NH, Jeong HJ, Kim HG. A pathological and immunohistochemical study of 9 cases of inflammatory fibroid polyp [in Korean]. Korean J Pathol. 1989. 23:20–28.30. Park SY, Kang HG, Lee HJ, Na GJ, Yi CY, Lee DH, et al. A case of inflammatory fibroid polyp of the cecum causing intussusception [in Korean]. Korean J Gastrointest Endosc. 2005. 30:281–285.31. Singh N, Harrison M, Rex DK. A survey of colonoscopic polypectomy practices among clinical gastroenterologists. Gastrointest Endosc. 2004. 60:414–418.32. Cipolletta L, Bianco MA, Rotondano G, Catalano M, Prisco A, De Simone T. Endoclip-assisted resection of large pedunculated colon polyps. Gastrointest Endosc. 1999. 50:405–406.33. Matsushita M, Takakuwa H, Matsubayashi Y, Kido M, Shimeno N, Okazaki K. Handcrafted two-channel colonoscope for grasping-forceps-assisted resection of giant pedunculated polyps. Gastrointest Endosc. 2005. 62:132–136.
Article34. Akahoshi K, Kojima H, Fujimaru T, Kondo A, Kubo S, Furuno T, et al. Grasping forceps assisted endoscopic resection of large pedunculated GI polypoid lesions. Gastrointest Endosc. 1999. 50:95–98.
Article35. Valentine JF. Double-channel endoscopic polypectomy technique for the removal of large pedunculated polyps. Gastrointest Endosc. 1998. 48:314–316.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Inflammatory Fibroid Polyp of the Stomach
- Colorectal Polyps : Endoscopic Diagnosis and Polypectomy
- A Case of Inflammatory Fibroid Polyp Presenting with Jejunal Bleeding
- Gastric Inflammatory Fibroid Polyp Resected by Endoscopic Submucosal Dissection
- A Pathological and Immunohistochemical Study of 9 Cases of Inflammatory Fibroid Polyp
