Symptomatic Posterior Mediastinal Angioleiomyoma
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Pusan National University School of Medicine, Busan, Korea. domini@pnu.edu
- 2Department of Radiology, Pusan National University School of Medicine, Busan, Korea.
- 3Department of Pathology, Pusan National University School of Medicine, Busan, Korea.
- KMID: 1793205
- DOI: http://doi.org/10.3349/ymj.2008.49.4.666
Abstract
- We report a case of a symptomatic angioleiomyoma in the left posterior mediastinum. A 66-year-old woman presented with left back and flank pain for 6 months. Chest computed tomography (CT) and magnetic resonance imaging (MRI) revealed a well-circumscribed 4.3cm round mass. The mass was initially diagnosed as nerve sheath tumor, because of her symptoms and its close location to the sympathetic trunk and intercostal nerve. It was uneventfully removed through video-assisted thoracoscopic surgery. The pathology revealed an angioleiomyoma.
Figure
-

Fig. 1 With MRI, this mass shows relatively homogeneous low SI on T1-WI (A) and high SI on T2-WI (B). Interlacing areas of iso-SI (arrows) and a well-defined peripheral low SI rim (arrowhead) are seen on T2-WI. Gadolinium-enhanced coronal T1-WI (C) show relatively homogeneous and strong enhancement with signal void tubular structures (arrow). MRI, magnetic resonance imaging; SI, signal intensity; WI, weighted image.
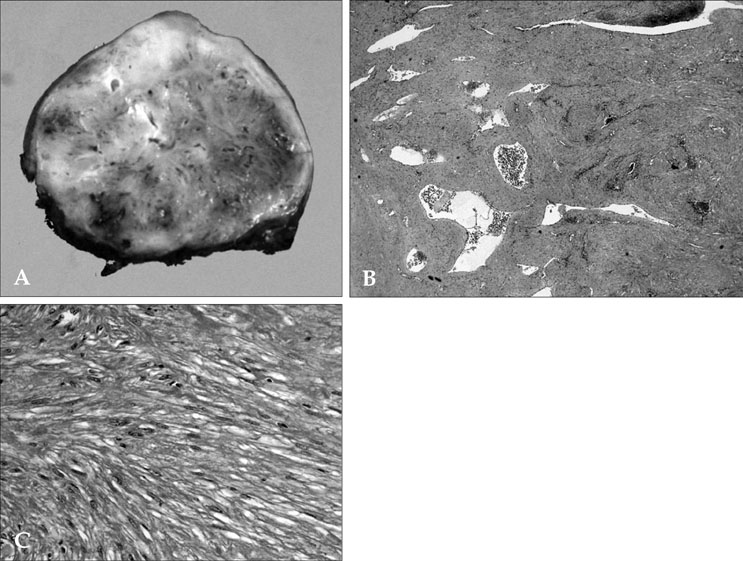
Fig. 2 Gross and microscopic findings of a well-demarcated and spherical resected tumor. The cut surface is brownish-white colored and sponge-like (A). The tumor mass is composed of well-differentiated smooth muscle cells and some dilated vascular channels with RBCs (B, H&E, × 40). Smooth muscle cells show no atypism and mitoses (C, H&E, × 400).
Reference
-
1. Duhig JT, Ayer JP. Vascular leiomyoma. A study of sixtyone cases. Arch Pathol. 1959. 68:424–430.2. Beissert M, Kenn W, Schultz G, Keberle M, Eck M, Hahn D. Hepatic angiomyoma: CT and MRI findings. Abdom Imaging. 2002. 27:40–42.3. Kunimatsu N, Kunimatsu A, Kojima K, Hirabayasi Y, Ohtomo K. A case of renal angioleiomyoma with rapid growing: CT findings with histopathological correlation. Radiat Med. 2004. 22:437–441.4. Matsuoka H, Nishio W, Sakamoto T, Harada H, Sashikata T, Tsubota N. Mediastinal angioleiomyoma. Ann Thorac Surg. 2002. 73:1653–1654.
Article5. Vrtik M, Larbalestier RI, Cameron D, Gupta A, Sinniah R. Giant superior mediastinal angioleiomyoma. J Thorac Cardiovasc Surg. 2004. 128:786–788.6. Yasuda A, Mizuno A, Mishima A, Sasaki S, Ochi N, Wakasugi T, et al. Posterior mediastinal angioleiomyoma report of a case. J Thorac Imaging. 2007. 22:363–365.7. Hwang JW, Ahn JM, Kang HS, Suh JS, Kim SM, Seo JW. Vascular leiomyoma of an extremity: MR imaging-pathology correlation. AJR Am J Roentgenol. 1998. 171:981–985.
Article
