Yonsei Med J.
2013 Sep;54(5):1143-1148. 10.3349/ymj.2013.54.5.1143.
Late-Presenting Congenital Diaphragmatic Hernia in Children: The Experience of Single Institution in Korea
- Affiliations
-
- 1Department of Pediatric Surgery, Yeouido St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea. jhjung@catholic.ac.kr
- KMID: 1793161
- DOI: http://doi.org/10.3349/ymj.2013.54.5.1143
Abstract
- PURPOSE
Late-presenting congenital diaphragmatic hernia (CDH) beyond the neonatal period is rare and often misdiagnosed, with delayed treatment.
MATERIALS AND METHODS
We retrospectively reviewed our experience with late-presenting CDH over 30 years at a single institution to determine the characteristics of late-presenting CDH for early diagnosis.
RESULTS
Seven patients had operations due to late-presenting CHD in our institution over 30 years. The patients' ages ranged from 2.5 months to 16 years. There were six boys and one girl. Five hernias were left-sided, one was right-sided and one was a retrosternal hernia. All patients had normal intestinal rotation. Non-specific gastrointestinal or respiratory symptoms and signs were usually presented. Intestinal malrotations were absent; therefore, only organs adjacent to the defect or relatively movable organs such as the small bowel and transverse colon were herniated. Two cases were accompanied by stomach herniation with the volvulus and liver, respectively. The duration from presentation to diagnosis varied from 5 days to 1 year. Diagnoses were made by chest X-ray, upper gastrointestinal series and chest computed tomography. All patients underwent primary repair with interrupted non-absorbable sutures by a transabdominal approach. None had postoperative complications. The follow-up period in six patients ranged from 4 months to 20 years (median 3.8 years). There was no recurrence in any of the patients on follow-up.
CONCLUSION
A high index of suspicion is important for the diagnosis of late-presenting CDH because it can be a life-threatening condition such as CDH with a gastric volvulus. Early diagnosis and appropriate treatment can lead to a good prognosis.
MeSH Terms
Figure
-
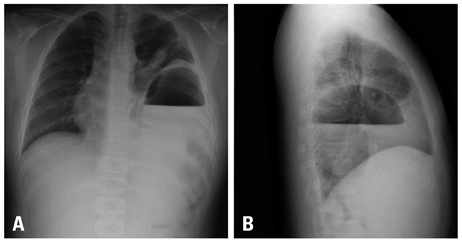
Fig. 1 Preoperative chest radiographs (A: posteroanterior, B: lateral) in case 6 showing a large gastric air fluid level and air within the bowel loops herniated into the left chest.
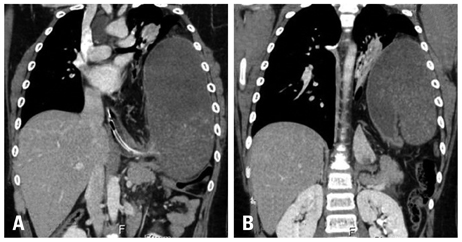
Fig. 2 Chest CT scan in case 6 showing a herniated stomach with huge distension passing a NG tube (A) and organoaxial torsion of the stomach (B). NG, nasogastric.
Reference
-
1. Day B. Late appearance of Bochdalek hernia. Br Med J. 1972; 1:786.
Article2. Wiseman NE, MacPherson RI. "Acquired" congenital diaphragmatic hernia. J Pediatr Surg. 1977; 12:657–665.
Article3. Elhalaby EA, Abo Sikeena MH. Delayed presentation of congenital diaphragmatic hernia. Pediatr Surg Int. 2002; 18:480–485.
Article4. Bagłaj M. Late-presenting congenital diaphragmatic hernia in children: a clinical spectrum. Pediatr Surg Int. 2004; 20:658–669.
Article5. Reiss I, Schaible T, van den Hout L, Capolupo I, Allegaert K, van Heijst A, et al. Standardized postnatal management of infants with congenital diaphragmatic hernia in Europe: the CDH EURO Consortium consensus. Neonatology. 2010; 98:354–364.
Article6. Gentili A, Giuntoli L, Bacchi Reggiani ML, Masciopinto F, Lima M, Baroncini S. Neonatal congenital diaphragmatic hernia: respiratory and blood-gas derived indices in choosing surgical timing. Minerva Anestesiol. 2012; 78:1117–1125.7. Hosgor M, Karaca I, Karkiner A, Ucan B, Temir G, Erdag G, et al. Associated malformations in delayed presentation of congenital diaphragmatic hernia. J Pediatr Surg. 2004; 39:1073–1076.
Article8. Chang SW, Lee HC, Yeung CY, Chan WT, Hsu CH, Kao HA, et al. A twenty-year review of early and late-presenting congenital Bochdalek diaphragmatic hernia: are they different clinical spectra? Pediatr Neonatol. 2010; 51:26–30.
Article9. Baerg J, Kanthimathinathan V, Gollin G. Late-presenting congenital diaphragmatic hernia: diagnostic pitfalls and outcome. Hernia. 2012; 16:461–466.
Article10. Muzzafar S, Swischuk LE, Jadhav SP. Radiographic findings in late-presenting congenital diaphragmatic hernia: helpful imaging findings. Pediatr Radiol. 2012; 42:337–342.
Article11. Waseem M, Quee F. A wheezing child: breath sounds or bowel sounds? Pediatr Emerg Care. 2008; 24:304–306.12. Strunk T, Simmer K, Kikiros C, Patole S. Late-onset right-sided diaphragmatic hernia in neonates-case report and review of the literature. Eur J Pediatr. 2007; 166:521–526.
Article13. Weber TR, Tracy T Jr, Bailey PV, Lewis JE, Westfall S. Congenital diaphragmatic hernia beyond infancy. Am J Surg. 1991; 162:643–646.
Article14. Ayala JA, Naik-Mathuria B, Olutoye OO. Delayed presentation of congenital diaphragmatic hernia manifesting as combined-type acute gastric volvulus: a case report and review of the literature. J Pediatr Surg. 2008; 43:E35–E39.
Article15. Vandy FC, Landrum JE, Gerig NR, Prahlow JA. Death due to late-presenting congenital diaphragmatic hernia in a 2-year-old child. Am J Forensic Med Pathol. 2008; 29:75–79.
Article16. al-Salem AH. Intrathoracic gastric volvulus in infancy. Pediatr Radiol. 2000; 30:842–845.
Article17. Schimpl G, Fotter R, Sauer H. Congenital diaphragmatic hernia presenting after the newborn period. Eur J Pediatr. 1993; 152:765–768.
Article18. Sharma S, Gopal SC. Gastric volvulus with perforation in association with congenital diaphragmatic hernia. Indian J Pediatr. 2004; 71:948.19. Beckmann KR, Nozicka CA. Congenital diaphragmatic hernia with gastric volvulus presenting as an acute tension gastrothorax. Am J Emerg Med. 1999; 17:35–37.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Late Presenting Congenital Diaphragmatic Hernia
- Unilateral Congenital Diaphragmatic Eventration Mimicking Congenital Diaphragmatic Hernia
- Diagnostic Considerations of Late Presenting Congenital Diaphragmatic Hernia in Children: Single Center Experience
- A Case of Sliding Hiatal Hernia associated with Bochdalek Hernia Repair
- Cardiac Arrest Due to Unrecognized Congenital Diaphragmatic Hernia
