Sympathetic Nerve Reconstruction for Compensatory Hyperhidrosis after Sympathetic Surgery for Primary Hyperhidrosis
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Gangnam Severance Hospital, Yonsei University, College of Medicine, Seoul, Korea. dylee@yuhs.ac
- KMID: 1792931
- DOI: http://doi.org/10.3346/jkms.2010.25.4.597
Abstract
- We performed sympathetic nerve reconstruction using intercostal nerve in patients with severe compensatory hyperhidrosis after sympathetic surgery for primary hyperhidrosis, and analyzed the surgical results. From February 2004 to August 2007, sympathetic nerve reconstruction using intercostal nerve was performed in 19 patients. The subjected patients presented severe compensatory hyperhidrosis after thoracoscopic sympathetic surgery for primary hyperhidrosis. Reconstruction of sympathetic nerve was performed by thoracoscopic surgery except in 1 patient with severe pleural adhesion. The median interval between the initial sympathetic surgery and sympathetic nerve reconstruction was 47.2 (range: 3.5-110.7) months. Compensatory sweating after the reconstruction surgery improved in 9 patients, and 3 out of them had markedly improved symptoms. Sympathetic nerve reconstruction using intercostal nerve may be one of the useful surgical options for severe compensatory hyperhidrosis following sympathetic surgery for primary hyperhidrosis.
Keyword
MeSH Terms
Figure
-
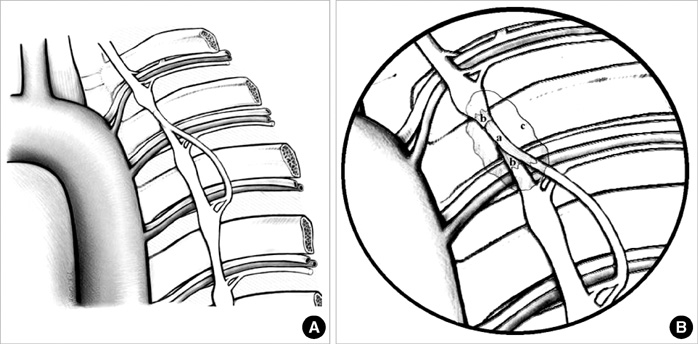
Fig. 1 (A) Illustration of operative field. (B) Magnified view of nerve anastomosis. The distal part of the intercostal nerve (a) was placed between the proximal and distal ends of the exposed sympathetic nerve (b) to contact with the sympathetic nerve and intercostal nerve, and fibrin sealant (c) was applied to the contact surface of the sympathetic and intercostal nerve.
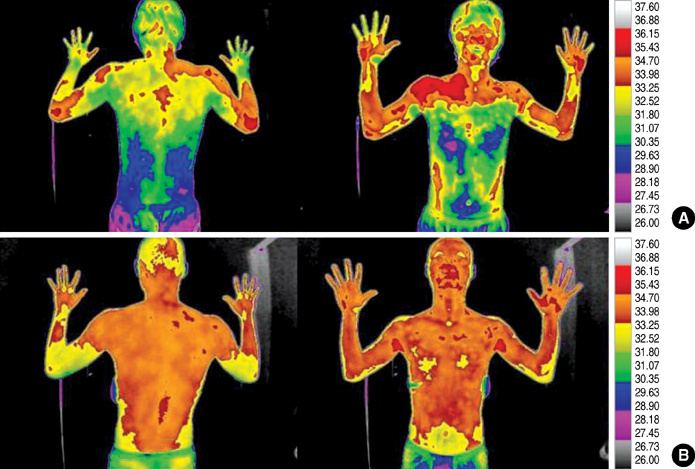
Fig. 2 (A) and (B) are infrared thermographic image obtained before sympathetic reconstruction surgery and after postoperative 3 months, respectively. Preoperative and postoperative digital infrared thermographic imaging show the apparent thermal change in chest and back.
Cited by 1 articles
-
Alternative Surgical Methods in Patients with Recurrent Palmar Hyperhidrosis and Compensatory Hyperhidrosis
Hee Suk Jung, Doo Yun Lee, Joon Suk Park
Yonsei Med J. 2018;59(2):345-348. doi: 10.3349/ymj.2018.59.2.345.
Reference
-
1. Adar R, Kurchin A, Zweig A, Mozes M. Palmar hyperhidrosis and its surgical treatment: a report of 100 cases. Ann Surg. 1977. 186:34–41.2. Lin TS, Fang HY. Transthoracic endoscopic sympathectomy in the treatment of palmar hyperhidrosis with emphasis on perioperative management (1,360 case analyses). Surg Neurol. 1999. 52:453–457.3. Kux EF. Endoscopic resection of the autonomic nervous system of the thoracic cavity. Rev Esp Tuberc. 1951. 20:19–24.4. Shachor D, Jedeikin R, Olsfanger D, Bendahan J, Sivak G, Freund U. Endoscopic transthoracic sympathectomy in the treatment of primary hyperhidrosis. A review of 290 sympathectomies. Arch Surg. 1994. 129:241–244.5. Fox AD, Hands L, Collin J. The results of thoracoscopic sympathetic trunk transection for palmar hyperhidrosis and sympathetic ganglionectomy for axillary hyperhidrosis. Eur J Vasc Endovasc Surg. 1999. 17:343–346.
Article6. Drott C, Gothberg G, Claes G. Endoscopic transthoracic sympathectomy: an efficient and safe method for the treatment of hyperhidrosis. J Am Acad Dermatol. 1995. 33:78–81.
Article7. Lee DY, Yoon YH, Shin HK, Kim HK, Hong YJ. Needle thoracic sympathectomy for essential hyperhidrosis: intermediate-term follow-up. Ann Thorac Surg. 2000. 69:251–253.
Article8. Fredman B, Zohar E, Shachor D, Bendahan J, Jedeikin R. Video-assisted transthoracic sympathectomy in the treatment of primary hyperhidrosis: friend or foe? Surg Laparosc Endosc Percutan Tech. 2000. 10:226–229.
Article9. Lin TS, Wang NP, Huang LC. Pitfalls and complication avoidance associated with transthoracic endoscopic sympathectomy for primary hyperhidrosis (analysis of 2200 cases). Int J Surg Investig. 2001. 2:377–385.10. Gossot D, Galetta D, Pascal A, Debrosse D, Caliandro R, Girard P, Stern JB, Grunenwald D. Long-term results of endoscopic thoracic sympathectomy for upper limb hyperhidrosis. Ann Thorac Surg. 2003. 75:1075–1079.
Article11. Adar R. Compensatory sweating after upper dorsal sympathectomy. J Neurosurg. 1979. 51:424–425.
Article12. Shih GJ. Compensatory sweating after upper dorsal sympathectomy. J Neurosurg. 1979. 51:425.
Article13. Kao MC. Video endoscopic sympathectomy using a fiberoptic CO2 laser to treat palmar hyperhidrosis. Neurosurgery. 1992. 30:131–135.
Article14. Gossot D, Toledo L, Fritsch S, Celerier M. Thoracoscopic sympathectomy for upper limb hyperhidrosis: looking for the right operation. Ann Thorac Surg. 1997. 64:975–978.
Article15. Noppen M, Herregodts P, D'Haese J, D'Haens J, Vincken W. A simplified T2-T3 thoracoscopic sympathicolysis technique for the treatment of essential hyperhidrosis: short-term results in 100 patients. J Laparoendosc Surg. 1996. 6:151–159.16. Bonjer HJ, Hamming JF, du Bois N, van Urk H. Advantages of limited thoracoscopic sympathectomy. Surg Endosc. 1996. 10:721–723.
Article17. Drott C, Claes G. Hyperhidrosis treated by thoracoscopic sympathicotomy. Cardiovasc Surg. 1996. 4:788–791.
Article18. Chou SH, Kao EL, Lin CC, Chang YT, Huang MF. The importance of classification in sympathetic surgery and a proposed mechanism for compensatory hyperhidrosis: experience with 464 cases. Surg Endosc. 2006. 20:1749–1753.
Article19. Schoeller T, Ohlbauer M, Wechselberger G, Piza-Katzer H, Margreiter R. Successful immediate phrenic nerve reconstruction during mediastinal tumor resection. J Thorac Cardiovasc Surg. 2001. 122:1235–1237.
Article20. Telaranta T. Secondary sympathetic chain reconstruction after endoscopic thoracic sympathicotomy. Eur J Surg Suppl. 1998. 580:17–18.
Article21. Miura J, Doita M, Miyata K, Yoshiya S, Kurosaka M, Yamamoto H. Horner's syndrome caused by a thoracic dumbbell-shaped schwannoma: sympathetic chain reconstruction after a one-stage removal of the tumor. Spine. 2003. 28:E33–E36.
Article22. Terris DJ, Fee WE Jr. Current issues in nerve repair. Arch Otolaryngol Head Neck Surg. 1993. 119:725–731.
Article23. Parker G, White T, Jenkins R. Surgical repair of extratemporal facial nerve: a comparison of suture repair and microfibrillar collagen repair. Laryngoscope. 1984. 94:950–953.24. Gosk J, Knakiewicz M, Wiacek R, Reichert P. The use of the fibrin glue in the peripheral nerves reconstructions. Polim Med. 2006. 36:11–15.25. Suri A, Mehta VS, Sarkar C. Microneural anastomosis with fibrin glue: an experimental study. Neurol India. 2002. 50:23–26.26. Beris A, Lykissas M, Korompilias A, Mitsionis G. End-to-side nerve repair in peripheral nerve injury. J Neurotrauma. 2007. 24:909–916.
Article27. Sotereanos DG, Seaber AV, Urbaniak JR, Spiegel DA, Sotereanos D, Anthony DC. Reversing nerve-graft polarity in a rat model: the effect on function. J Reconstr Microsurg. 1992. 8:303–307.
Article28. Stromberg BV, Vlastou C, Earle AS. Effect of nerve graft polarity on nerve regeneration and function. J Hand Surg Am. 1979. 4:444–445.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Thoracoscopic Sympathetic Nerve Reconstruction with using an Intercostal Nerve Graft after Thoracoscopic Sympathetic Clipping for Facial Hyperhidrosis
- Alternative Surgical Methods in Patients with Recurrent Palmar Hyperhidrosis and Compensatory Hyperhidrosis
- Limited Sympathetic Nervelipping of T2 Sympathetic Chain Block for Essential Hyperhidrosis
- Thoracic Sympathetic Ganglion Block for a Patient with Hyperhidrosis
- Ramicotomy of T2, 3 Sympathetic Ganglia for Palmar Hyperhidrosis
