A Ten-year Follow-up of a Case with Gastric Adenoma Accompanied with Gastritis Cystica Profunda Treated by Endoscopic Submucosal Dissection
- Affiliations
-
- 1Department of Internal Medicine, Bundang Jesaeng General Hospital, Seongnam, Korea. parkjs@dmc.or.kr
- 2Department of Pathology, Bundang Jesaeng General Hospital, Seongnam, Korea.
- KMID: 1792836
- DOI: http://doi.org/10.4166/kjg.2012.59.5.366
Abstract
- Gastritis cystica profunda (GCP) is an uncommon hyperplastic benign lesion, and histologically characterized by hyperplasia and cystic dilatation of the gastric glands extending into the submucosal layer. GCP usually occurs at a gastroenterostomy site, although it can occasionally be found in an unoperated stomach. GCP is thought to be a possible precancerous lesion, since a few early gastric cancers associated with it were reported. Herein, we report a case of gastric adenoma associated with GCP in an unoperated patient. The sizes of both the GCP and adenoma overlying it have increased during a 10 year follow-up period. Adenoma on the latest biopsy showed low grade dysplasia, and it was successfully treated by endoscopic submucosal dissection.
MeSH Terms
Figure
-

Fig. 1 (A) Stomach CT finding (3 years ago). It showed an about 3×2.7 cm sized relatively well-defined low density cystic mass (arrow) in the submucosal layer with partly enhanced mucosal portion at the lesser curvature side of the low body. (B) Endoscopic ultrasonography findings. A multiseptated homogenous anechoic lesion (arrow) originating from the third layer accompanied focal wall thickening (arrow head) of the first layer.
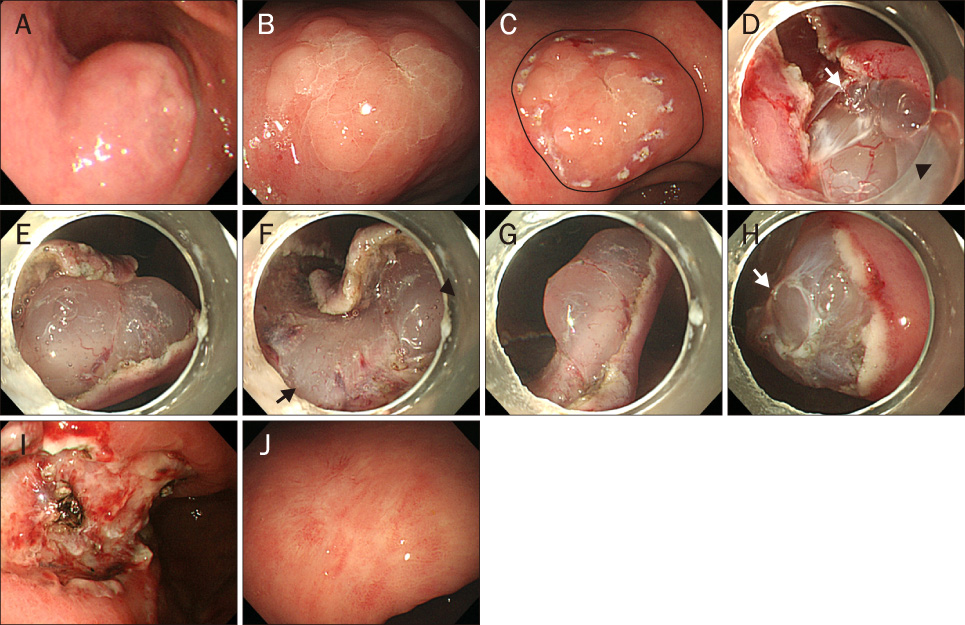
Fig. 2 Endoscopic images. (A) Endoscopy showed an about 3 cm sized slight translucent submucosal tumor accompanied with whitish geographic mucosal lesion on its surface at the lesser curvature side of the lower body (3 years ago). (B) It showed an 4 cm sized submucosal tumor at the same site, but the mucosal lesion has extended (current). (C) Marking. Circumferential marking were made at several points at least 2 mm apart from the outline of mucosal adenomatous lesion by APC within the margin of gastritis cystica profunda (solid line). (D) Submucosal injection and marginal incision. After submucosal injection with Unylone® to help lift the mucosal lesion, marginal incision was done around the lesion using an IT knife 2. Fibrous septum (arrow) and cystic lesion (arrow head) of gastritis cystica profunda were shown after the incision. (E) Submucosal dissection. It showed cystic lesion of remaining gastritis cystica profunda during the dissection. (F) Remaining deep layer of normal submucosa (arrow) and cystic lesion (arrow head) were shown during dissection. (G) Remaining cystic lesion of gastritis cystica profunda after dissection. (H) Partialy resected submucosal cystic lesion with fibrous septal structure (arrow). (I) A post-endoscopic submucosal dissection (ESD) active ulcer without remnant cystic lesion (the day after ESD). (J) A post-ESD ulcer scar without remnant cystic lesion or recurrence of adenoma (6 months later after ESD).

Fig. 3 (A) Gross finding. The endoscopic submucosal dissection (ESD) specimen measured 3.2×2.5×0.3 cm. It contained an elevated nodular lesion. (B) Microscopic finding. The ESD specimen showed many cystic glands lined by flattend epithelium within the mucosa and low grade tubular adenoma in the surface (H&E, ×40). (C) A low grade tubular adenoma was found and the mucosa showed cystic dilatation of gastric glands (H&E, ×100).
Reference
-
1. Littler ER, Gleibermann E. Gastritis cystica polyposa. (Gastric mucosal prolapse at gastroenterostomy site, with cystic and infiltrative epithelial hyperplasia). Cancer. 1972. 29:205–209.2. Franzin G, Novelli P. Gastritis cystica profunda. Histopathology. 1981. 5:535–547.3. Kim W, Park SC, Lee JY, et al. A case of gastric adenocarcinoma diagnosed after being followed up as submucosal tumor for 10 years. Korean J Gastroenterol. 2001. 37:291–295.4. Iwanaga T, Koyama H, Takahashi Y, Taniguchi H, Wada A. Diffuse submucosal cysts and carcinoma of the stomach. Cancer. 1975. 36:606–614.5. Chakrovorty RC, Schatzki PF. Gastric cystic polyposis. Am J Dig Dis. 1975. 20:981–989.6. Cho HJ, Kim JE, Jeong BJ, et al. A case of gastric adenocarcinoma arising from gastritis cystica profunda. Korean J Gastrointest Endosc. 2004. 28:237–241.7. Chung IK, Kim EJ, Kim DJ, et al. Clinical significance of endoscopic Ultrasonography in gastritis cystica polyposa. Korean J Gastrointest Endosc. 2001. 22:195–210.8. Moon SY, Kim KO, Park SH, et al. Gastritis cystica profunda accompanied by multiple early gastric cancers. Korean J Gastroenterol. 2010. 55:325–330.9. Aoyagi K, Koufuji K, Yano S, et al. Two cases of cancer in the remnant stomach derived from gastritis cystica polyposa. Kurume Med J. 2000. 47:243–248.10. Song YL, Park JY, Kim YB, et al. A case of gastritis cystica profunda associated with high grade tubular adenoma. Korean J Gastroenterol. 2004. 43:52–55.11. Park CH, Park JM, Jung CK, et al. Early gastric cancer associated with gastritis cystica polyposa in the unoperated stomach treated by endoscopic submucosal dissection. Gastrointest Endosc. 2009. 69:e47–e50.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Gastritis Cystica Profunda Showing Giant Gastric Mucosal Fold
- A Case of Gastritis Cystica Profunda Presenting with a Submucosal Cystic Tumor
- A Case of Gastric Inverted Hyperplastic Polyp Found with Gastritis Cystica Profunda and Early Gastric Cancer
- A Case of Gastritis Cystica Profunda Associated with High Grade Tubular Adenoma
- Gastritis Cystica Profunda: A case report
