Macular Hole Formation after Pars Plana Vitrectomy for the Treatment of Valsalva Retinopathy: A Case Report
- Affiliations
-
- 1Department of Ophthalmology, Kyung Hee University Hospital, Kyung Hee University School of Medicine, Seoul, Korea. hwkwak@khu.ac.kr
- 2Department of Ophthalmology, Kangwon National University School of Medicine, Chuncheon, Korea.
- KMID: 1792099
- DOI: http://doi.org/10.3341/kjo.2014.28.1.91
Abstract
- We report a case of complete surgical resolution of Valsalva retinopathy that manifested as a premacular hemorrhage involving a membrane followed by a macular hole (MH) resulting from the first vitrectomy. A 20-year-old female patient was referred to our hospital due to sudden vision loss in the left eye. Her best-corrected visual acuity (BCVA) in the left eye was hand motion. Fundus photographs and optical coherence tomography (OCT) revealed a premacular hemorrhage. Nine weeks later, the BCVA in the left eye had returned to 20 / 100 and the premacular hemorrhage had completely resolved, but residual sub-internal limiting membrane deposits and a preretinal membrane were present. The preretinal membrane was removed by core vitrectomy and preretinal membrane peeling, but the foveal deposits could not be excised. Two weeks after the first vitrectomy, the deposits resolved spontaneously, but a full-thickness MH was present. Six months after a second vitrectomy with fluid-gas exchange, the BCVA in the left eye had improved to 20 / 25 and OCT showed that the MH had closed. This case illustrates the possibility of MH formation following vitrectomy for Valsalva retinopathy.
Keyword
MeSH Terms
Figure
-
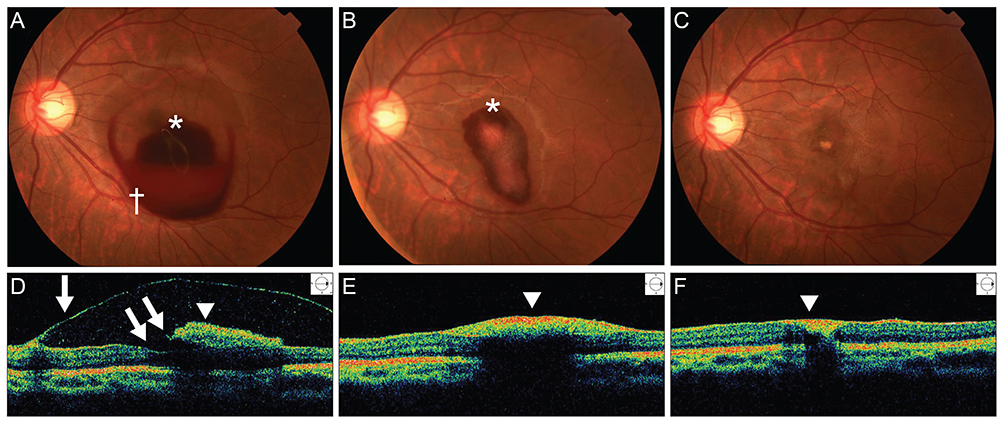
Fig. 1 (A) A fundus photograph of the left eye shows a dome-shaped sub-internal limiting membrane (ILM) hemorrhage (white asterisk) and a sub-hyaloid hemorrhage located anterior and inferotemporal to the sub-ILM hemorrhage (white cross) at initial presentation. Note the "double ring" sign with the "inner ring" caused by the sub-ILM hemorrhage and the "outer ring" caused by the sub-hyaloid hemorrhage. (B) After four weeks, a fundus photograph showed spontaneous absorption of the sub-hyaloid hemorrhage, but the sub-ILM hemorrhage remained. (C) After nine weeks, the sub-ILM and sub-hyaloid hemorrhages were almost completely resolved, and a focal yellowish lesion was observed on the fovea. (D) The Time-domain optical coherence tomography (OCT) at the initial presentation revealed a premacular hemorrhage with hyperreflective ILM (white arrowhead) and a hyporeflective sub-hyaloid membrane (white arrow). The foveal contour was intact (double arrow). (E) After four weeks, OCT showed resolution of the premacular hemorrhage with a thick preretinal membrane. (F) After nine weeks, the premacular hemorrhage was completely resolved, but a hyperreflective, thick preretinal membrane (white arrowhead) remained.
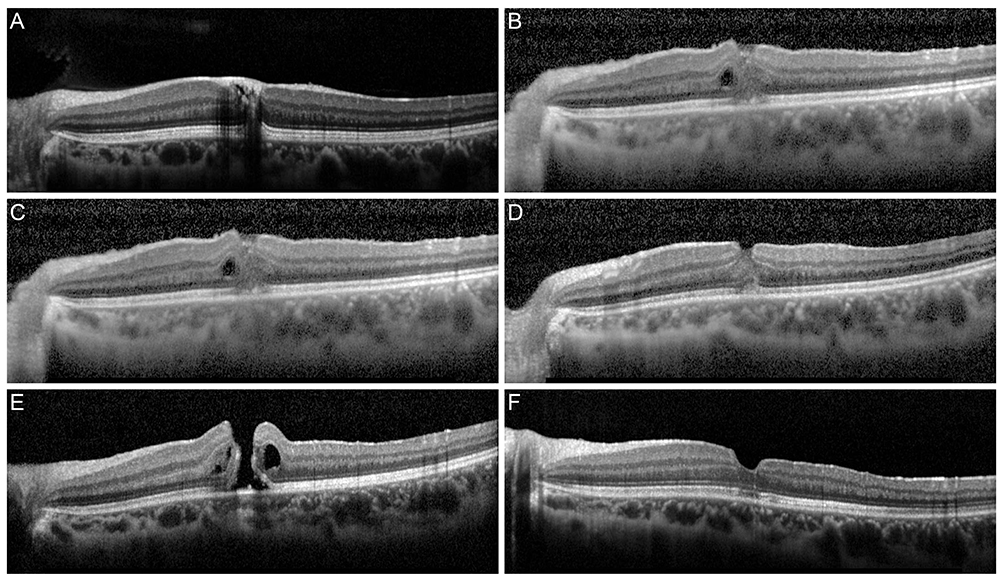
Fig. 2 Serial spectral domain-optical coherence tomography images before and after pars plana vitrectomy. The macular hole was not identified immediately after the first operation but was observed after resolution of the sub-internal limiting membrane deposits at two weeks after the first surgery. (A) Before 1st operation, (B) 1 day after 1st operation, (C) 4 day after 1st operation, (D) 7 day after 1st operation, (E) 14 day after 1st operation, and (F) 14 day after 2nd operation.
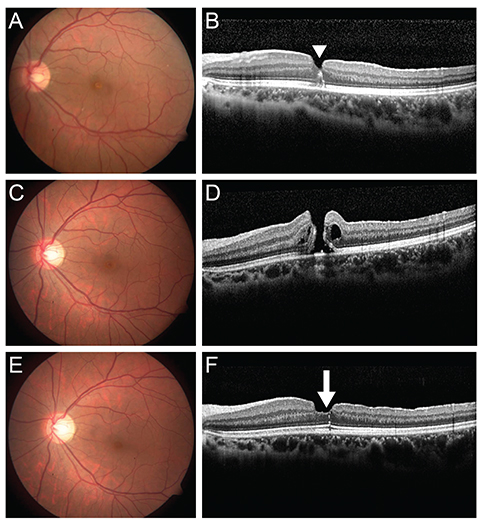
Fig. 3 (A,B) Fundus photograph and spectral domain-optical coherence tomography (SD-OCT) images after the initial pars plana vitrectomy. SD-OCT revealed hemosiderin-like deposits (arrowhead) of the fovea. (C,D) Fundus photograph and SD-OCT images before secondary pars plana vitrectomy. SD-OCT showed a full-thickness macular hole. (E,F) Six months after the second surgery, the macular hole was completely closed with minimal scarring of the photoreceptor inner/outer segment junction (arrow), as determined by SD-OCT.
Reference
-
1. Duane TD. Valsalva hemorrhagic retinopathy. Am J Ophthalmol. 1973; 75:637–642.2. Gass JD. Stereoscopic atlas of macular diseases: diagnosis and treatment. 4th ed. St. Louis: Mosby;1997. p. 752–754.3. Roberts DK, MacKay KA. Microhemorrhagic maculopathy associated with aerobic exercise. J Am Optom Assoc. 1987; 58:415–418.4. Friberg TR, Braunstein RA, Bressler NM. Sudden visual loss associated with sexual activity. Arch Ophthalmol. 1995; 113:738–742.5. De Crecchio G, Pacente L, Alfieri MC, Greco GM. Valsalva retinopathy associated with a congenital retinal macrovessel. Arch Ophthalmol. 2000; 118:146–147.6. Choi SW, Lee SJ, Rah SH. Valsalva retinopathy associated with fiberoptic gastroenteroscopy. Can J Ophthalmol. 2006; 41:491–493.7. Kwok AK, Lai TY, Chan NR. Epiretinal membrane formation with internal limiting membrane wrinkling after Nd:YAG laser membranotomy in valsalva retinopathy. Am J Ophthalmol. 2003; 136:763–766.8. De Maeyer K, Van Ginderdeuren R, Postelmans L, et al. Sub-inner limiting membrane haemorrhage: causes and treatment with vitrectomy. Br J Ophthalmol. 2007; 91:869–872.9. Durukan AH, Kerimoglu H, Erdurman C, et al. Long-term results of Nd:YAG laser treatment for premacular subhyaloid haemorrhage owing to Valsalva retinopathy. Eye (Lond). 2008; 22:214–218.10. Koh HJ, Kim SH, Lee SC, Kwon OW. Treatment of subhyaloid haemorrhage with intravitreal tissue plasminogen activator and C3F8 gas injection. Br J Ophthalmol. 2000; 84:1329–1330.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Vitreous Surgery for Macular Hole
- The Clinical Evaluation of Pars Plana Vitrectomy in various Ocular Disease
- Pars Plana Vitrectomy in Pars Planitis and Posterior Uveitis
- Pars Plana Vitrectomy in Pars Planitis and Posterior Uveitis
- Delayed Sealing of Macular Hole after Vitrectomy with Silicone Oil Tamponade
