The Relationship between Higher-order Aberrations and Amblyopia Treatment in Hyperopic Anisometropic Amblyopia
- Affiliations
-
- 1Department of Ophthalmology, Inje University Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea. jiwoong_chang@paik.ac.kr
- KMID: 1792095
- DOI: http://doi.org/10.3341/kjo.2014.28.1.66
Abstract
- PURPOSE
To investigate the relationship between higher-order aberrations (HOAs) and amblyopia treatment in children with hyperopic anisometropic amblyopia.
METHODS
The medical records of hyperopic amblyopia patients with both spherical anisometropia of 1.00 diopter (D) or more and astigmatic anisometropia of less than 1.00 D were reviewed retrospectively. Based on the results of the amblyopia treatment, patients were divided into two groups: treatment successes and failures. Using the degree of spherical anisometropia, subjects were categorized into mild, moderate, or severe groups. Ocular, corneal, and internal HOAs were measured using a KR-1W aberrometer at the initial visit, and at 3-month, 6-month, and 12-month follow-ups.
RESULTS
The results of the 45 (21 males and 24 females) hyperopic anisometropic amblyopia patients who completed the 12-month follow-up examinations were analyzed. The mean patient age at the initial visit was 70.3 months. In total, 28 patients (62.2%) had successful amblyopia treatments and 17 patients (37.8%) failed treatment after 12 months. Among the patient population, 24 (53.3%) had mild hyperopic anisometropia and 21 (46.7%) had moderate hyperopic anisometropia. When comparing the two groups (i.e., the success and failure groups), ocular spherical aberrations and internal spherical aberrations in the amblyopic eyes were significantly higher in the failure group at every follow-up point. There were no significant differences in any of the HOAs between mild and moderate cases of hyperopic anisometropia at any follow-up. When the amblyopic and fellow eyes were compared between the groups there were no significant differences in any of the HOAs.
CONCLUSIONS
HOAs, particularly ocular spherical aberrations and internal spherical aberrations, should be considered as reasons for failed amblyopia treatment.
MeSH Terms
-
Aged
Amblyopia/complications/physiopathology/*therapy
Anisometropia/complications/physiopathology/*therapy
Cornea/*pathology/physiopathology
*Eyeglasses
Female
Follow-Up Studies
Humans
Hyperopia/complications/physiopathology/*therapy
Male
Middle Aged
Refraction, Ocular/*physiology
Retrospective Studies
Treatment Outcome
*Visual Acuity
Figure
-
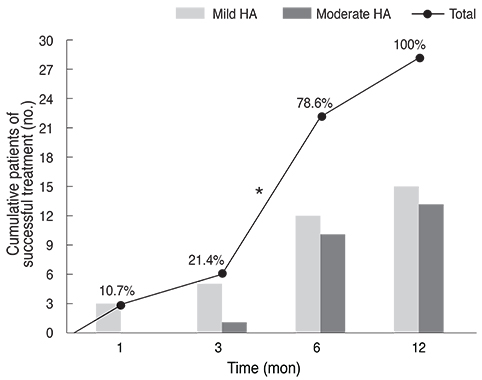
Fig. 1 Compiled patients of successful amblyopia treatment. Asterisk indicates that this follow-up period had the highest success rate among the total follow-up periods in both mild hyperopic anisometropia (HA) and moderate HA. The indicated percentages (%) are proportions of cumulative patients who had successful treatments compared to all of patients with successful treatments at each follow-up.
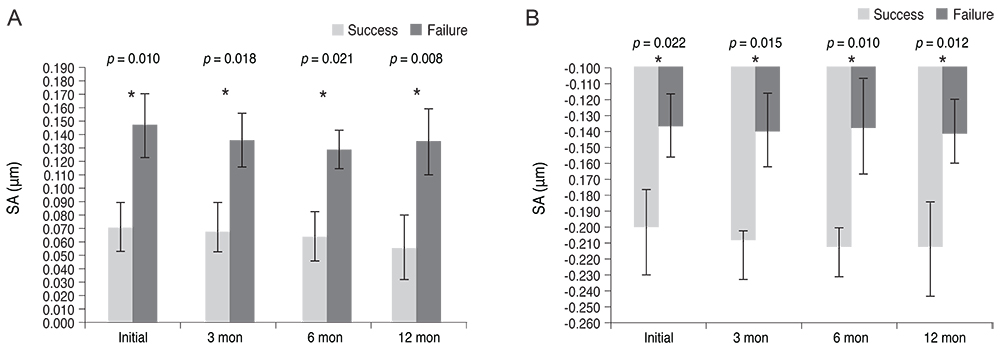
Fig. 2 Comparisons of ocular and internal spherical aberrations (SAs) in amblyopic eyes according to the results of amblyopia treatment (A, ocular SA root mean square [RMS]; B, internal SA RMS). When comparing the two groups (success and failure groups), the ocular SA and internal SA of amblyopic eyes were significantly higher in the failure group at every follow-up (*p < 0.05, statistically significant, Mann-Whitney U-test).
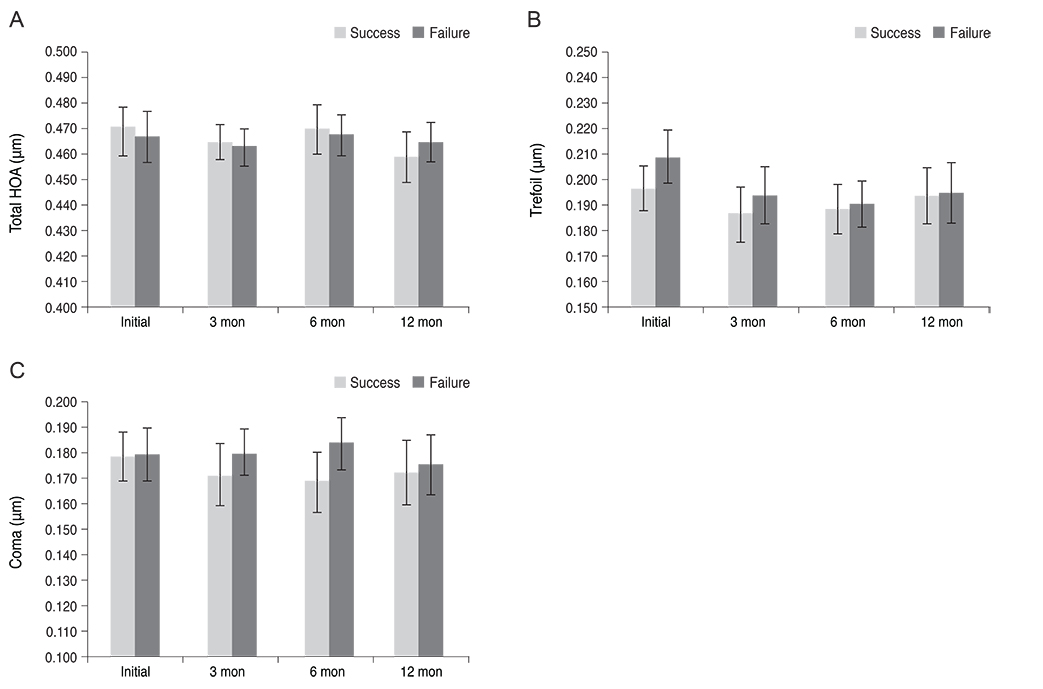
Fig. 3 Comparisons of ocular total higher-order aberrations (HOAs), ocular trefoil, and ocular coma of amblyopic eyes according to the results of amblyopia treatment (A, ocular total HOA root mean square [RMS]; B, ocular trefoil RMS; C, ocular coma RMS). There were no significant differences in the ocular total HOAs, trefoil, or coma of the amblyopic eyes between the success and failure group (Mann-Whitney U-test).

Fig. 4 Comparisons of ocular higher-order aberrations (HOAs) between amblyopic and fellow eyes in the failed amblyopia treatment group (A, ocular total HOA root mean square [RMS]; B, ocular trefoil RMS; C, ocular coma RMS; D, ocular spherical aberration [SA] RMS). There were no significant differences in the ocular total HOAs, trefoil, coma, or SA between the amblyopic eyes and fellow eyes (Mann-Whitney U-test).
Reference
-
1. Von Noorden GK. Binocular vision and ocular motility. 6th ed. St. Louis: Mosby;2002. p. 246–251.2. Flom MC, Bedell HE. Identifying amblyopia using associated conditions, acuity, and nonacuity features. Am J Optom Physiol Opt. 1985; 62:153–160.3. Pediatric Eye Disease Investigator Group. The clinical profile of moderate amblyopia in children younger than 7 years. Arch Ophthalmol. 2002; 120:281–287.4. Woodruff G, Hiscox F, Thompson JR, Smith LK. Factors affecting the outcome of children treated for amblyopia. Eye (Lond). 1994; 8(Pt 6):627–631.5. Yoon GY, Williams DR. Visual performance after correcting the monochromatic and chromatic aberrations of the eye. J Opt Soc Am A Opt Image Sci Vis. 2002; 19:266–275.6. Rossi EA, Weiser P, Tarrant J, Roorda A. Visual performance in emmetropia and low myopia after correction of high-order aberrations. J Vis. 2007; 7:14.7. Pinero DP, Juan JT, Alio JL. Intrasubject repeatability of internal aberrometry obtained with a new integrated aberrometer. J Refract Surg. 2011; 27:509–517.8. Von Noorden GK. Amblyopia: a multidisciplinary approach. Proctor lecture. Invest Ophthalmol Vis Sci. 1985; 26:1704–1716.9. Preslan MW, Novak A. Baltimore Vision Screening Project: phase 2. Ophthalmology. 1998; 105:150–153.10. McMullen WH. Some points in anisometropia in discussion on problem in refraction. Trans Ophthalmol Soc UK. 1939; 59:119.11. Weakley DR Jr. The association between nonstrabismic anisometropia, amblyopia, and subnormal binocularity. Ophthalmology. 2001; 108:163–171.12. Hussein MA, Coats DK, Muthialu A, et al. Risk factors for treatment failure of anisometropic amblyopia. J AAPOS. 2004; 8:429–434.13. Taylor K, Powell C, Hatt SR, Stewart C. Interventions for unilateral and bilateral refractive amblyopia. Cochrane Database Syst Rev. 2012; 4:CD005137.14. Writing Committee for the Pediatric Eye Disease Investigator Group. Cotter SA, Foster NC, et al. Optical treatment of strabismic and combined strabismic-anisometropic amblyopia. Ophthalmology. 2012; 119:150–158.15. Lithander J, Sjostrand J. Anisometropic and strabismic amblyopia in the age group 2 years and above: a prospective study of the results of treatment. Br J Ophthalmol. 1991; 75:111–116.16. Flynn JT, Schiffman J, Feuer W, Corona A. The therapy of amblyopia: an analysis of the results of amblyopia therapy utilizing the pooled data of published studies. Trans Am Ophthalmol Soc. 1998; 96:431–450.17. Menon V, Chaudhuri Z, Saxena R, et al. Factors influencing visual rehabilitation after occlusion therapy in unilateral amblyopia in children. Indian J Med Res. 2005; 122:497–505.18. Kirwan C, O'Keefe M. Higher order aberrations in children with amblyopia. J Pediatr Ophthalmol Strabismus. 2008; 45:92–96.19. Liang J, Grimm B, Goelz S, Bille JF. Objective measurement of wave aberrations of the human eye with the use of a Hartmann-Shack wave-front sensor. J Opt Soc Am A Opt Image Sci Vis. 1994; 11:1949–1957.20. Prakash G, Sharma N, Chowdhary V, Titiyal JS. Association between amblyopia and higher-order aberrations. J Cataract Refract Surg. 2007; 33:901–904.21. Prakash G, Sharma N, Saxena R, et al. Comparison of higher order aberration profiles between normal and amblyopic eyes in children with idiopathic amblyopia. Acta Ophthalmol. 2011; 89:e257–e262.22. Zhao PF, Zhou YH, Wang NL, Zhang J. Study of the wavefront aberrations in children with amblyopia. Chin Med J (Engl). 2010; 123:1431–1435.23. Plech AR, Pinero DP, Laria C, et al. Corneal higher-order aberrations in amblyopia. Eur J Ophthalmol. 2010; 20:12–20.24. Young T. The bakerian lecture: on the mechanism of the eye. Phil Trans R Soc Lond. 1801; 91:23–88.25. Roorda A, Glasser A. Wave aberrations of the isolated crystalline lens. J Vis. 2003; 4:250–261.26. Wang L, Dai E, Koch DD, Nathoo A. Optical aberrations of the human anterior cornea. J Cataract Refract Surg. 2003; 29:1514–1521.27. Artal P, Berrio E, Guirao A, Piers P. Contribution of the cornea and internal surfaces to the change of ocular aberrations with age. J Opt Soc Am A Opt Image Sci Vis. 2002; 19:137–143.28. Hickenbotham A, Tiruveedhula P, Roorda A. Comparison of spherical aberration and small-pupil profiles in improving depth of focus for presbyopic corrections. J Cataract Refract Surg. 2012; 38:2071–2079.29. Guo H, Atchison DA, Birt BJ. Changes in through-focus spatial visual performance with adaptive optics correction of monochromatic aberrations. Vision Res. 2008; 48:1804–1811.30. Birkenfeld J, de Castro A, Ortiz S, et al. Contribution of the gradient refractive index and shape to the crystalline lens spherical aberration and astigmatism. Vision Res. 2013; 86:27–34.31. Sawides L, Gambra E, Pascual D, et al. Visual performance with real-life tasks under adaptive-optics ocular aberration correction. J Vis. 2010; 10:19.32. Navarro R, Moreno-Barriuso E, Bara S, Mancebo T. Phase plates for wave-aberration compensation in the human eye. Opt Lett. 2000; 25:236–238.33. Sabesan R, Jeong TM, Carvalho L, et al. Vision improvement by correcting higher-order aberrations with customized soft contact lenses in keratoconic eyes. Opt Lett. 2007; 32:1000–1002.34. Macrae SM, Schwiegerling J, Snyder R. Customized corneal ablation and super vision. J Refract Surg. 2000; 16:2 Suppl. S230–S235.
