Takayasu's Arteritis Treated by Percutaneous Transluminal Angioplasty with Stenting in the Descending Aorta
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. younhj@catholic.ac.kr
- 2Department of Radiology, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 1786902
- DOI: http://doi.org/10.3346/jkms.2008.23.3.551
Abstract
- A 17-yr-old young woman was referred to our hospital with a 2-yr history of claudication of the lower extremities and severe arterial hypertension. Physical examination revealed significantly different blood pressures between both arms (160/92 and 180/95 mmHg) and legs (92/61 and 82/57 mmHg). The hematological and biochemical values were within their normal ranges, except for the increased erythrocyte sedimentation rate (83 mm/hr) and C-reactive protein (6.19 mg/L). On 3- dimensional computed tomographic angiography, the ascending aorta, the aortic arch and its branches, and the thoracic and, descending aorta, but not the renal artery, were shown to be stenotic. The diagnosis of type IIb Takayasu's arteritis was made according to the new angiographic classification of Takayasu's arteritis, Takyasu conference 1994. Percutaneous transluminal angioplasty with stenting was performed on the thoracic and abdominal aorta. After the interventional procedures, the upper extremity blood pressure improved from 162/101 mmHg to 132/85 mmHg, respectively. She has been free of claudication and there have been no cardiac events during 2-yr of clinical follow-up.
Keyword
MeSH Terms
Figure
-
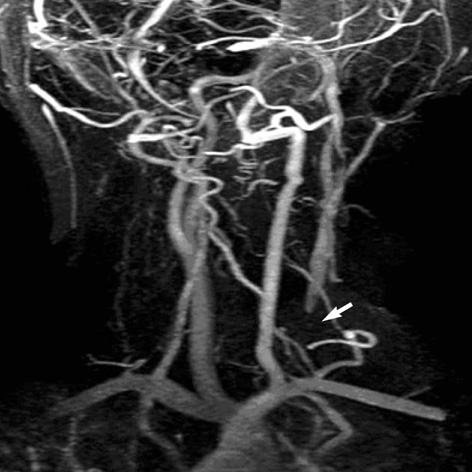
Fig. 1 Neck MR angiography demonstrates the cut-off, filling and near total occlusions (arrow) at the osteal lesions of the left common carotid artery on the posterior-anterior view.
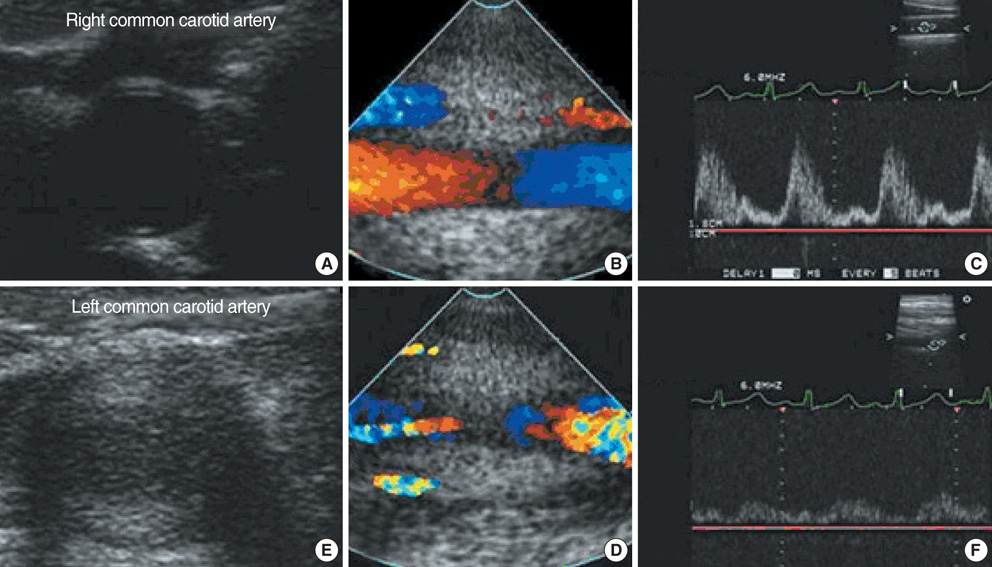
Fig. 2 The neck carotid Doppler sonogram. (A) Right common carotid artery shows normal luminal diameter without abnormalities. (B) and (C) Color flow doppler ultrasound scan (B) and spectral analysis (C) show a normal arterial flow in the right common carotid artery. (D) Left common carotid artery shows marked wall thickening and luminal narrowing. (E) and (F) Decreased blood flow on Color flow Doppler ultrasound scan (E) and decreased peak systolic pressure on spectral analysis (F) are noted in the left common carotid artery.
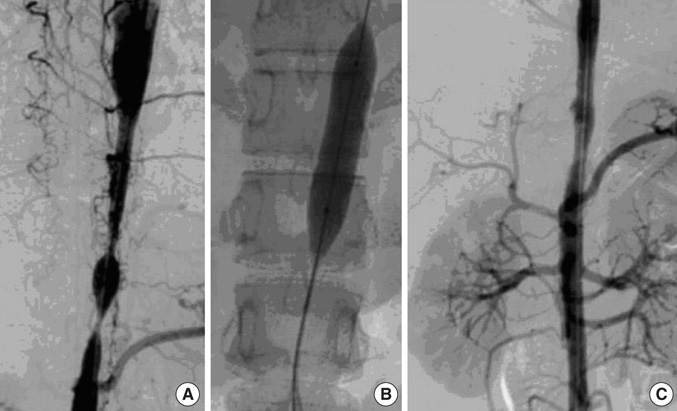
Fig. 3 (A) 3D-CT angiography shows focal stenosis in the descending aorta, but not the renal artery. (B) Percutaneous transluminal angioplasty was performed in the descending aorta using a 4.0/12 mm balloon catheter. (C) A 4.0/14 mm Niti-S stent in the aorta was inserted after ballooning.

Fig. 4 24-hr ABPM shows more than a 30 mmHg mean difference between the upper extremity blood pressure and the lower extremity blood pressure. (A) 24-hr ABPM of an arm before and after PTA (B) 24-hr ABPM of a leg before and after PTA. 24-hr ABPM, 24 hr-ambulatory blood pressure monitoring; PTA, percutaneous angioplasty.
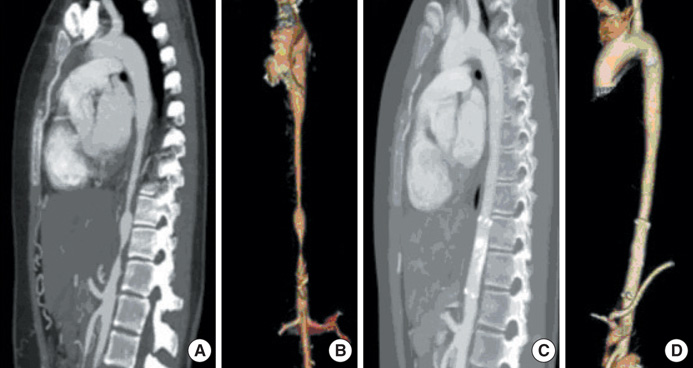
Fig. 5 (A) CT angiography shows the focal stenosis in the descending aorta beyond both renal arteries. (B) 3D reconstruction of CT angiography shows severe stenosis of the abdominal aorta, beyond both renal arteries. (C) After the insertion of a stent-graft, CT angiography shows the dilation of stenotic segments in the descending aorta. (D) 3D reconstruction of CT angiography after the insertion of a stent-graft.
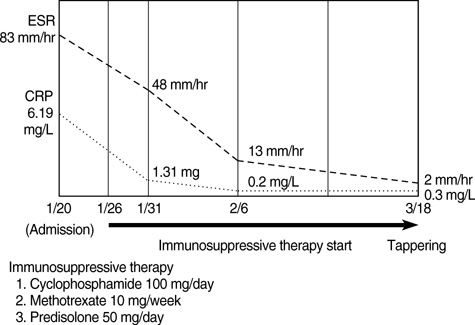
Fig. 6 Changes of ESR and CRP levels.
Reference
-
1. Ishikawa K, Maetani S. Long-term outcome for 120 Japanese patients with Takayasu\'s disease Clinical and statistical analysis of related prognostic factors. Circulation. 1994. 90:1855–1860.2. Sawada S, Tanigawa N, Kobayashi M, Morioka N, Kotani K, Senda T, Okuda Y, Ohta Y. Treatment of Takayasu's arteritis with self-expanding metallic stent (Giant-urco stent) in two patients. Cardiovasc Intervent Radiol. 1994. 17:102–105.
Article3. Moriwaki R, Noda M, Yajima M, Sharma BK, Numano F. Clinical manifestations of Takayasu arteritis in India and Japan--new classification of angiographic findings. Angiology. 1997. 48:369–379.4. Arend WP, Michel BA, Bloch DA, Hunder GG, Calabrese LH, Edworthy SM, Fauci AS, Leavitt RY, Lie JT, Rightfoot RW Jr, Masi AT, Mcshane DJ, Mills JA, Stevens MB, Wallace SL, Zvaifler NJ. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990. 33:1129–1134.
Article5. Hoffman GS, Ahmed AE. Surrogate markers of disease activity in patients with Takayasu arteritis. A preliminary report from The International Network for the Study of the Systemic Vasculitides (INSSYS). Int J Cardiol. 1998. 66:Suppl 1. S191–S194.6. Andrew J, Al-Nahhas A, Pennell DJ, Hossain MS, Davies KA, Haskard DO, Mason JC. Non-invasive imaging in the diagnosis and management of Takayasu's arteritis. Ann Rheum Dis. 2004. 63:995–1000.7. Noris M, Daina E, Gamba S, Bonazzola S, Remuzzi G. Interleukin-6 and RANTES in Takayasu arteritis a guide for therapeutic decisions? Circulation. 1999. 100:55–60.8. Choe YH, Han BK, Koh EM, Kim DK, Do YS, Lee WR. Takayasu's arteritis: assessment of disease activity with contrastenhanced MR imaging. Am J Roentgenol. 2000. 175:505–511.9. Park JH. Disease activity of Takayasu's arteritis. Korean Circ J. 2001. 31:1103–1105.
Article10. Shelhamer JH, Volkman DJ, Parrillo JE, Lawley TJ, Johnston MR, Fauci AS. Takayasu's arteritis and its therapy. Ann Intern Med. 1985. 103:121–126.
Article11. Hoffmann GS, Leavitt RY, Kerr GS, Rottem M, Sneller MC, Fauci AS. Treatment of glucocorticoid-resistant or relapsing Takayasu arteritis with methotrexate. Arthritis Rheum. 1994. 37:578–582.12. Della Rossa A, Tavoni A, Merlini G, Baldini C, Sebastiani M, Lombardi M, Neglia D, Bombardieri S. Two Takayasu arteritis patients successfully treated with infliximab: a potential disease-modifying agent? Rheumatology. 2005. 44:1074–1075.
Article13. Koh KK, Hwang HK, Kim PG, Lee SH, Cho SK, Kim SS, Han JJ, Lee YT, Park PW, Yoon DH. Isolated left main coronary ostial stenosis in Oriental people: operative, histopathologic and clinical findings in six patients. J Am Coll Cardiol. 1993. 21:369–373.
Article14. Pyun WB, Yoon YS, Park KJ, Kim SY, Shim WH. Carotid artery stenting in patients Takayasu's arteritis: early and long-term follow-up results. Korean Circ J. 2000. 30:592–598.15. Kerr GS, Hallahan CW, Giordano J, Leavitt RY, Fauci AS, Rottem M, Hoffman GS. Takayasu arteritis. Ann Intern Med. 1994. 120:919–929.
Article16. Tyagi S, Kaul UA, Nair M, Sethi KK, Arora R, Khalilullah M. Balloon angioplasty of the aorta in Takayasu's arteritis: initial and long-term results. Am Heart J. 1992. 124:876–882.
Article17. Giordano JM. Surgical treatment of Takayasu's arteritis. Int J Cardiol. 2000. 75:Suppl 1. S123–S128.
Article18. Bali HK, Jain S, Jain A, Sharma BK. Stent supported angioplasty in Takayasu arteritis. Int J Cardiol. 1998. 66:Suppl 1. S213–S217.
Article19. Gimenez-Roqueplo AP, Tomkiewicz E, La Batide-Alanore A, Moreau I, Paul JF, Raynaud A, Plouin PF. Stent treatment for pseudocoarctation and refractory hypertension in an elderly patient with Takayasu's arteritis. Nephrol Dial Transplant. 2000. 15:536–538.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of percutaneous transluminal angioplasty in Takayasu arteritis
- Percutaneous transluminal coronary angioplasty for ostial stenosis of the left coronary artery
- One Case of Percutaneous Transluminal Angioplasty of Renal Artery Stenosis Caused by Takayasu's Arteritis
- A Case of Takayasu's Arteritis : Managed with Percutaneous Transluminal Angioplasty
- Stenting of the Left Main Coronary Artery in a Patient With Takayasu's Arteritis
