Isolated and Complex Scimitar Vein Anomalies and Their Differentiation from the Meandering Right Pulmonary Vein
- KMID: 1786212
- DOI: http://doi.org/10.3349/ymj.2007.48.6.973
Abstract
- PURPOSE: Four pediatric patients with isolated (the adult form) and complex (the infantile form) scimitar vein anomalies were reviewed and compared with patients with meandering right pulmonary veins. MATERIALS AND METHODS: From January 1990 to December 2006, 4 female patients, aged 2 days to 3.5 years, with isolated and complex scimitar vein anomalies were retrospectively studied. The clinical features, chest radiographs, echocardiography, magnetic resonance imaging, magnetic resonance angiography, computer tomography, bronchography, cardiac catheterization with angiography, surgery, and autopsy were reviewed to substantiate the diagnosis of isolated and complex scimitar vein anomalies. RESULTS: Clinical manifestations were lung infections with radiographic scimitar signs in 4 patients (3 right; 1 left), respiratory distress, congestive heart failure, pulmonary hypertension and/or cyanosis in 3 patients, dextrocardia, heterotaxy, and/or right atrial isomerism in 2 patients, as well as dextroversion, right bronchial isomerism, bronchial stenosis, and/or sepsis in 1 patient. Two patients with right atrial isomerism expired. CONCLUSION: The clinical discrimination between scimitar vein anomaly with and without cardiovascular and bronchopulmonary malformations is crucial for the outcomes vary.
Keyword
MeSH Terms
Figure
-
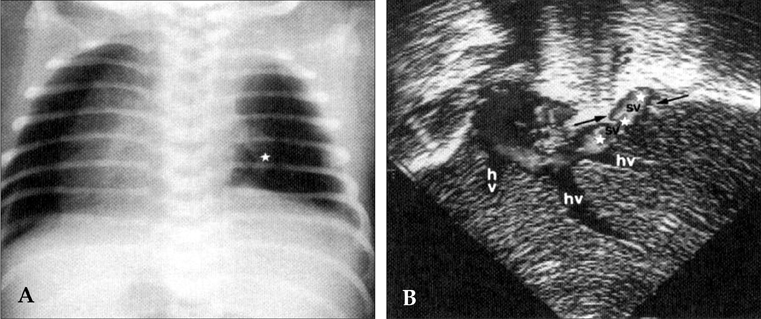
Fig. 1 Patient 3, a 4-day-old female baby. (A) Plain chest radiograph showed a positive scimitar sign (white star) that was left-sided. (B) Echocardiography with Doppler showed drainage of this left-sided scimitar vein (sv) into the hepatic vein (hv).
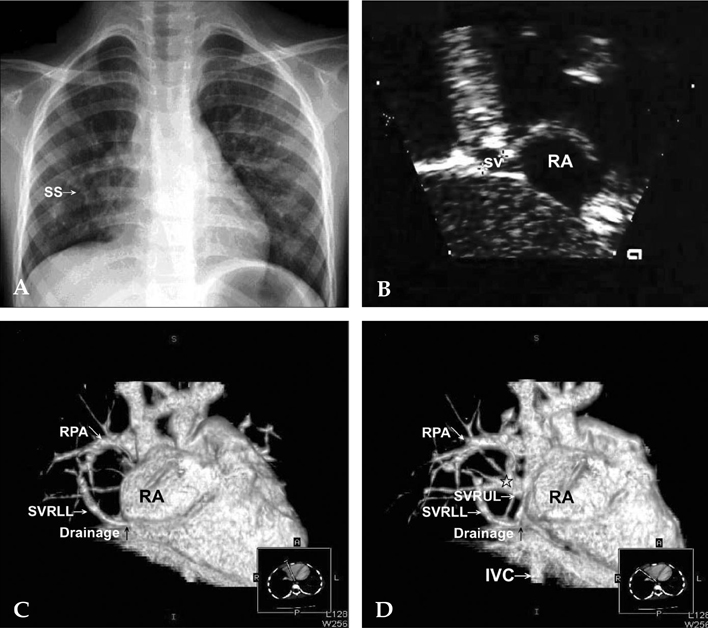
Fig. 2 Patient 4, a 3.5-year-old girl. (A) Plain chest radiograph showed loss of cardiac silhouette at the right lower cardiac border with a positive scimitar sign (SS). (B) Two-dimensional echocardiography showed drainage of the scimitar vein (SV) into the right atrium (RA). (C and D) Chest computer tomography showed two abnormal vessels draining the right upper lobe (SVRUL) and the right lower lobe (SVRLL), and converging as a right-sided scimitar vein. This vessel drained to the junction of the inferior vena cava (IVC) and the right atrium (RA) above the diaphragm (black arrow). RPA denotes right pulmonary artery. The black open star indicates that one set of the right pulmonary veins was draining normally to the left atrium.
Reference
-
1. Cooper G. Case of malformation of the thoracic viscera: Consisting of imperfect development of right lung and transposition of the heart. London Med Gazzette. 1836. 18:600–601.2. Chassinat R. Observation d'anomalies anatomiques remarquables de l'appareil circulatoire, avec hepatocele congeniale, n'ayant donne lieu pendant la vie a aucun symptom particulier. Arch Gen Med. 1836. 11:80–84.3. Halasz NA, Halloran KH, Liebow AA. Bronchial and arterial anomalies with drainage of the right lung into the inferior vena cava. Circulation. 1956. 14:826–846.
Article4. Neill CA, Ferencz C, Sabiston DC, Sheldon H. The familial occurrence of hypoplastic right lung with systemic arterial supply and venous drainage "scimitar syndrome". Bull Johns Hopkins Hosp. 1960. 107:1–21.5. Clements BS, Warner JO. Pulmonary sequestration and related congenital bronchopulmonary-vascular malformations: nomenclature and classification based on anatomical and embryological considerations. Thorax. 1987. 42:401–408.
Article6. Clements BS, Warner JO, Shinebourne EA. Congenital bronchopulmonary vascular malformations: clinical application of a simple anatomical approach in 25 cases. Thorax. 1987. 42:409–416.
Article7. Lee ML, Tsao LY, Chaou WT, Yang AD, Yeh KT, Wang JK, et al. Revisit on congenital bronchopulmonary vascular malformations: a haphazard branching theory of malinosculations and its clinical classification and implication. Pediatr Pulmonol. 2002. 33:1–11.
Article8. Morgan JR, Forker AD. Syndrome of hypoplasia of the right lung and dextroposition of the heart: "scimitar sign" with normal pulmonary venous drainage. Circulation. 1971. 43:27–30.
Article9. Kanemoto N, Sugiyama T, Hirose S, Goto Y. A case with pseudo-scimitar syndrome: "scimitar sign" with normal pulmonary venous drainage. Jpn Circ J. 1987. 51:642–646.
Article10. Herer B, Jaubert F, Delaisements C, Huchon G, Chretien J. Scimitar sign with normal pulmonary venous drainage and anomalous inferior vena cava. Thorax. 1988. 43:651–652.
Article11. Cukier A, Kavakama J, Teixeira LR, Terra-Filho M, Vargas FS. Scimitar sign with normal pulmonary venous drainage and systemic arterial supply. Scimitar syndrome or bronchopulmonary sequestration? Chest. 1994. 105:294–295.
Article12. Partridge JB, Osborne JM, Slaughter RE. Scimitar etcetera-the dysmorphic right lung. Clin Radiol. 1988. 39:11–19.13. Oakley D, Naik D, Verel D, Rajan S. Scimitar vein syndrome: report of nine new cases. Am Heart J. 1984. 107:596–598.
Article14. Pearl W. Scimitar variant. Pediatr Cardiol. 1987. 8:139–141.
Article15. Tumbarello R, Abbruzzese PA, Meloni G, Porcu M, Martelli V, Sanna A. A variant of the scimitar syndrome with stenosed drainage of the inferior vena cava. Am Heart J. 1991. 121:616–618.
Article16. Rose C, Vosshenrich R. Incomplete scimitar syndrome. Cardiol Young. 2002. 12:389–390.
Article17. Freedom RM, Burrows PE, Moes CA. "Horseshoe" lung: report of five new cases. AJR Am J Roentgenol. 1986. 146:211–215.
Article18. Frank JL, Poole CA, Rosas G. Horseshoe lung: clinical, pathologic, and radiologic features and a new plain film finding. AJR Am J Roentgenol. 1986. 146:217–226.
Article19. Dupuis C, Rémy J, Rémy-Jardin M, Coulomb M, Brevière GM, Ben Laden S. The "horseshoe" lung: six new cases. Pediatr Pulmonol. 1994. 17:124–130.
Article20. Clements BS, Warner JO. The crossover lung segment: congenital malformation associated with a variant of scimitar syndrome. Thorax. 1987. 42:417–419.
Article21. Goodman LR, Jamshidi A, Hipona FA. Meandering right pulmonary vein simulating the scimitar syndrome. Chest. 1972. 62:510–512.
Article22. Tortoriello TA, Vick GW, Chung T, Bezold LI, Vincent JA. Meandering right pulmonary vein to the left atrium and inferior vena cava: the first case with associated anomalies. Tex Heart Inst J. 2002. 29:319–323.23. Takeda S, Imachi T, Arimitsu K, Minami M, Hayakawa M. Two cases of scimitar variant. Chest. 1994. 105:292–293.
Article24. Collins DR, Shea PM, Vieweg WV. Idiopathic prominence of pulmonary veins on chest x-ray. Angiology. 1982. 33:613–616.
Article25. Salazar-Mena J, Salazar-Gonzalez J, Salazar-Gonzalez E. Meandering right pulmonary vein: a case of scimitar variant. Pediatr Radiol. 1999. 29:578–580.
Article26. Kriss VM, Woodring JH, Cottrill CM. "Meandering" pulmonary veins: report of a case in an asymptomatic 12-year-old girl. J Thorac Imaging. 1995. 10:142–145.27. Gazzaniga AB, Matloff JM, Harken DE. Anomalous right pulmonary venous drainage into the inferior vena cava and left atrium. J Thorac Cardiovasc Surg. 1969. 57:251–254.
Article28. Mohiuddin SM, Levin HS, Runco V, Booth RW. Anomalous pulmonary venous drainage: a common trunk empting into the left atrium and inferior vena cava. Circulation. 1966. 34:46–51.29. Geggel RL. Scimitar syndrome associated with partial anomalous pulmonary venous connection at the supracardiac, cardiac, and infracardiac levels. Pediatr Cardiol. 1993. 14:234–237.
Article30. Honey M. Anomalous pulmonary venous drainage of right lung to inferior vena cava ('scimitar syndrome'): clinical spectrum in older patients and role of surgery. Q J Med. 1977. 184:463–483.31. Juraszek AL, Cohn H, Van Praagh R, Van Praagh S. Isolated left-sided scimitar vein connecting all left pulmonary veins to the right inferior vena cava. Pediatr Cardiol. 2005. 26:846–847.
Article32. Mas C, Goh TH, Wilkinson JL. New interventional therapeutic approach for dual drainage of the scimitar vein. Catheter Cardiovasc Interv. 2000. 51:192–195.
Article33. Lee ML, Yang SC, Yang AD. Transcatheter occlusion of the isolated scimitar vein anomaly camouflaged under dual pulmonary venous drainage of the right lung by the Amplatzer Ductal Occluder. Int J Cardiol. 2007. 115:e90–e93.
Article34. Dupuis C, Charaf LA, Brevière GM, Abou P. "Infantile" form of the scimitar syndrome with pulmonary hypertension. Am J Cardiol. 1993. 71:1326–1330.
Article35. Dupuis C, Charaf LA, Brevière GM, Abou P, Rémy-Jardin M, Helmius G. The "adult" form of the scimitar syndrome. Am J Cardiol. 1992. 70:502–507.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Angiographic Findings of an Isolated Meandering Pulmonary Vein: A Case Report
- A Rare Case of Scimitar Syndrome Accompanied with an Imperforate Anus in a Newborn
- Familial Chromosome No. 9 Pericentic Inversion Producing Scimitar Syndrome
- A Case of Surgically Corrected-Combined form of Total Anomalous Pulmonary Venous Return
- Levoatriocardinal Vein Combined with Pulmonary Venous Varix Mimicking Arteriovenous Malformations: A Case Report
