Bronchial Atresia Associated with Spontaneous Pneumothorax : Report of A Case
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, College of Medicine, Inha University, Incheon, Korea. khkim@inha.ac.kr
- 2Department of Diagnostic Radiology, College of Medicine, Inha University, Incheon, Korea.
- 3Department of Pathology, Medical School, Jeju National University, Jeju, Korea.
- KMID: 1785710
- DOI: http://doi.org/10.3346/jkms.2004.19.1.142
Abstract
- A 32-yr-old male patient with recurrent pneumothorax associated with bronchial atresia of the subsegmental branch of the posterior segmental bronchus of the right upper lobe was successfully treated with right upper lobectomy. Before surgery, the bronchial atresia with pneumothorax was suspected on the chest radiograph and CT scans, which showed the findings of bronchocele with localized hyperinflation of the right upper lobe. The examination of surgical specimen from the resected right upper lobe suggests that the cause of the recurrent pneumothorax was the rupture of the subpleural bullae in the hyperinflated lung segment distal to the atretic bronchus.
Keyword
MeSH Terms
Figure
-
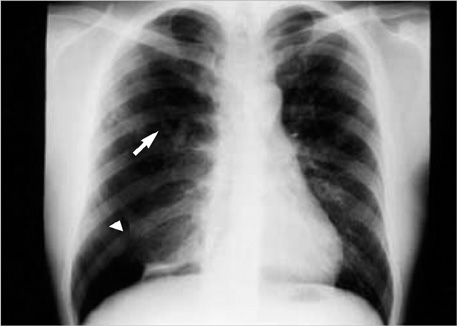
Fig. 1 A posteroanterior chest radiograph reveals increased radiolucency along with overinflated lung parenchyma and sparse vasculature in the upper half of the right lung. Also noted v-shaped branching opacity is in the right parahilar area (arrow). Pneumothorax is associated in the right lower pleural cavity (arrow head).

Fig. 2 Chest CT scan shows a branching soft tissue density in the region of the posterior segment of the right upper lobe with marked decrease in attenuation and vascularity. The subsegmental branch of the posterior segmental bronchus could not be traced distal to this (arrow) posterior segmental bronchus.
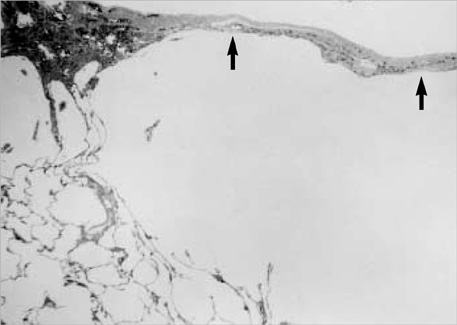
Fig. 3 Microscopic findings of the posterior segment of the right upper lobe include subpleural bullae (arrows) which are surrounded by focally overinflated alveoli. (Hematoxylin-Eosin stain×12.5).
Reference
-
1. Ferguson TB Jr, Ferguson TB. Sabiston DC, Spencer FC, editors. Congenital lesions of the lung and emphysema. Surgery of the chest. 1995. 6th ed. Philadelphia: WB Saunders Company;834.2. Montague NT, Shaw RR. Bronchial atresia. Ann Thorac Surg. 1974. 18:337–345.
Article3. Meng RL, Jensik RJ, Faber LP, Matthew GR, Kittle CF. Bronchial atresia. Ann Thorac Surg. 1978. 25:184–192.
Article4. Jederlinic PJ, Sicilian LS, Baigmelman W, Gaensler EA. Congenital bronchial atresia. A report of 4 cases and a review of the literature. Medicine. 1986. 73–83.5. Berkman N, Bar-Ziv J, Breuer R. Recurrent spontaneous pneumothorax associated with bronchial atresia. Respir Med. 1996. 90:307–309.
Article6. Kim SH, Jang IS, Kim BK, Ouck CD, Kim JW. Bronchial atresia with collapse of the right upper lobe. A case report. Korean J Thorac Cardiovasc Surg. 1997. 30:843–845.7. Ward S, Morcos SK. Congenital bronchial atresia - presentation of three cases and a pictorial review. Clin Radiol. 1999. 54:144–148.8. Nordstrom CR, Kane GC, Wechsler RJ, Salazar AM, Cohn HE, Faber JL. Bronchial atresia with relapsing pulmonary infection in a middle-aged man. Respir Care. 2001. 46:601–603.
