Clin Orthop Surg.
2014 Jun;6(2):190-195. 10.4055/cios.2014.6.2.190.
Does Well Maintained Graft Provide Consistent Return to Play after Medial Ulnar Collateral Ligament Reconstruction of the Elbow Joint in Elite Baseball Players?
- Affiliations
-
- 1Department of Orthopaedic Surgery, Konkuk University School of Medicine, Seoul, Korea. airbahng@naver.com
- KMID: 1784666
- DOI: http://doi.org/10.4055/cios.2014.6.2.190
Abstract
- BACKGROUND
Several studies have reported the clinical outcomes of medial ulnar collateral ligament (MUCL) reconstruction of the elbow joint in throwing athletes, including the rate of return to sports. However, little has been known about the imaging outcomes after MUCL reconstruction. The aim of this study is to report the clinical and imaging outcomes after MUCL reconstruction using figure of eight fashion in the elite and professional baseball players.
METHODS
This study included 17 baseball players, who underwent MUCL reconstruction between July 2007 and May 2010. The average follow-up period was 48.6 months. Imaging assessment consisted of preoperative plain and stress radiographs, magnetic resonance imaging, and postoperative serial ultrasonography. The clinical assessments were composed of visual analogue scale (VAS) for pain, range of motion, and the Conway scale.
RESULTS
The mean VAS score was 6.4 (range, 3 to 8) preoperatively and 2.2 (range, 0 to 4) postoperatively (p < 0.05). There were nine players (53%) classified as excellent who returned to sports at the same or higher level compared to preinjury. Serial ultrasonography revealed well-maintained grafts at 3 and 12 months in all of the players. Five out of 17 players showed decreased echogenecity in the common flexor tendon at 3 months, which was considered as remaining tissue swelling and resolved completely at 12 months.
CONCLUSIONS
All grafts are well-maintained until 12-months based on the ultrasonographic findings, although only 53% of the players returned to preinjury level.
MeSH Terms
Figure
-
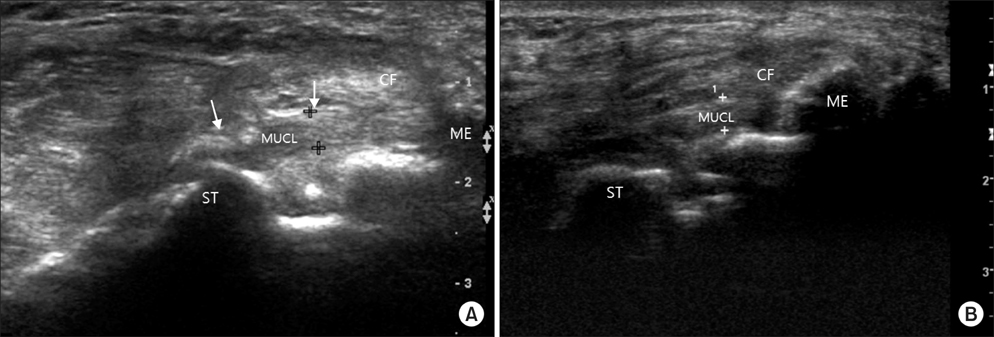
Fig. 1 Postoperative ultrasonography showing patent MUCL graft at 3 months (A) and 12 months (B). The thickness of the incorporated graft is consistent at each evaluation (3.8 mm). MUCL: medial ulnar collateral ligament, ME: medial epicondyle, ST: sublime tubercle of ulna, CF: common flexor tendon.
Reference
-
1. Ciccotti MG, Jobe FW. Medial collateral ligament instability and ulnar neuritis in the athlete's elbow. Instr Course Lect. 1999; 48:383–391.2. Hechtman KS, Tjin-A-Tsoi EW, Zvijac JE, Uribe JW, Latta LL. Biomechanics of a less invasive procedure for reconstruction of the ulnar collateral ligament of the elbow. Am J Sports Med. 1998; 26(5):620–624.3. Morrey BF, An KN. Articular and ligamentous contributions to the stability of the elbow joint. Am J Sports Med. 1983; 11(5):315–319.4. Schwab GH, Bennett JB, Woods GW, Tullos HS. Biomechanics of elbow instability: the role of the medial collateral ligament. Clin Orthop Relat Res. 1980; (146):42–52.5. Elattrache NS, Thompson B. Clinical impact of elbow magnetic resonance imaging. Oper Tech Sports Med. 1997; 5(1):33–36.6. Jobe FW, Nuber G. Throwing injuries of the elbow. Clin Sports Med. 1986; 5(4):621–636.7. Conway JE, Jobe FW, Glousman RE, Pink M. Medial instability of the elbow in throwing athletes: treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am. 1992; 74(1):67–83.8. Azar FM, Andrews JR, Wilk KE, Groh D. Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med. 2000; 28(1):16–23.9. Morrey BF, An KN. Functional anatomy of the ligaments of the elbow. Clin Orthop Relat Res. 1985; (201):84–90.10. Morrey BF, Tanaka S, An KN. Valgus stability of the elbow: a definition of primary and secondary constraints. Clin Orthop Relat Res. 1991; (265):187–195.11. Jobe FW, Stark H, Lombardo SJ. Reconstruction of the ulnar collateral ligament in athletes. J Bone Joint Surg Am. 1986; 68(8):1158–1163.12. Dines JS, Yocum LA, Frank JB, ElAttrache NS, Gambardella RA, Jobe FW. Revision surgery for failed elbow medial collateral ligament reconstruction. Am J Sports Med. 2008; 36(6):1061–1065.13. Thompson WH, Jobe FW, Yocum LA, Pink MM. Ulnar collateral ligament reconstruction in athletes: muscle-splitting approach without transposition of the ulnar nerve. J Shoulder Elbow Surg. 2001; 10(2):152–157.14. Feltner ME. Three-dimensional interactions in a two-segment kinetic chain. Part II: application to the throwing arm in baseball pitching. Int J Sports Biomech. 1989; 5(4):420–450.15. Fleisig GS, Barrentine SW. Biomechanical aspects of the elbow in sports. Sports Med Arthrosc. 1995; 3(3):149–159.16. Hechtman KS, Zvijac JE, Wells ME, Botto-van Bemden A. Long-term results of ulnar collateral ligament reconstruction in throwing athletes based on a hybrid technique. Am J Sports Med. 2011; 39(2):342–347.17. Rohrbough JT, Altchek DW, Hyman J, Williams RJ 3rd, Botts JD. Medial collateral ligament reconstruction of the elbow using the docking technique. Am J Sports Med. 2002; 30(4):541–548.18. Smith GR, Altchek DW, Pagnani MJ, Keeley JR. A muscle-splitting approach to the ulnar collateral ligament of the elbow: neuroanatomy and operative technique. Am J Sports Med. 1996; 24(5):575–580.19. Ahmad CS, ElAttrache NS. Valgus extension overload syndrome and stress injury of the olecranon. Clin Sports Med. 2004; 23(4):665–676.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Ulnar Collateral Ligament Reconstruction Techniques in the Elbow of Sports Players
- Management of Ulnar Collateral Ligament Injuries in Overhead Athletes
- Ulnar collateral ligament repair in professional baseball players
- Gravity Valgus Stress Ultrasonographic Assessment of Ulnar Collateral Ligament Injury among Baseball Players
- Ulnar Collateral Ligament Tear Combined with Medial Epicondylitis of the Elbow
