CT Findings of Colonic Complications Associated with Colon Cancer
- Affiliations
-
- 1Department of Radiology, Cheonan Hospital, Soonchunhyang University, Cheonan 330-720, Korea. rad2000@hanmail.net
- 2Department of Pathology, Cheonan Hospital, Soonchunhyang University, Cheonan 330-720, Korea.
- KMID: 1783198
- DOI: http://doi.org/10.3348/kjr.2010.11.2.211
Abstract
- A broad spectrum of colonic complications can occur in patients with colon cancer. Clinically, some of these complications can obscure the presence of underlying malignancies in the colon and these complications may require emergency surgical management. The complications of the colon that can be associated with colon cancer include obstruction, perforation, abscess formation, acute appendicitis, ischemic colitis and intussusception. Although the majority of these complications only rarely occur, familiarity with the various manifestations of colon cancer complications will facilitate making an accurate diagnosis and administering prompt management in these situations. The purpose of this pictorial essay is to review the CT appearance of the colonic complications associated with colon cancer.
MeSH Terms
-
Abdominal Abscess/complications/radiography
Adult
Aged
Aged, 80 and over
Appendicitis/complications/radiography
Colitis, Ischemic/complications/radiography
Colon/*radiography
Colonic Diseases/complications/radiography
Colonic Neoplasms/*complications/*radiography
Female
Humans
Intestinal Diseases/*complications/*radiography
Intestinal Obstruction/complications/radiography
Intussusception/complications/radiography
Male
Middle Aged
Tomography, X-Ray Computed/*methods
Figure
-
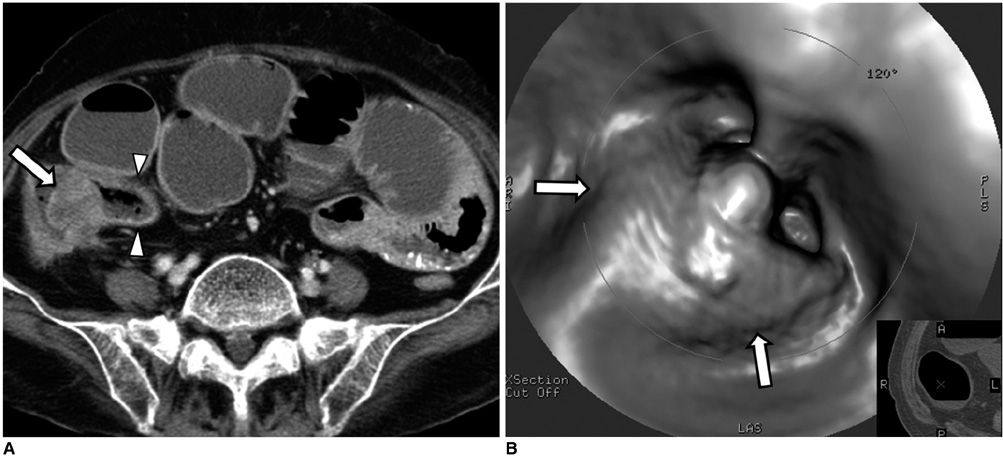
Fig. 1 80-year-old woman with adenocarcinoma near ileocecal valve and she presented with small bowel obstruction. A. Contrast-enhanced axial CT scan shows polypoid mass obstructing ileocecal valve area (arrow). Note dilated small bowel loops, including terminal ileum (arrowheads). B. Endoluminal 3D view from CT colonography shows polypoid mass at ileocecal valve area (arrows).
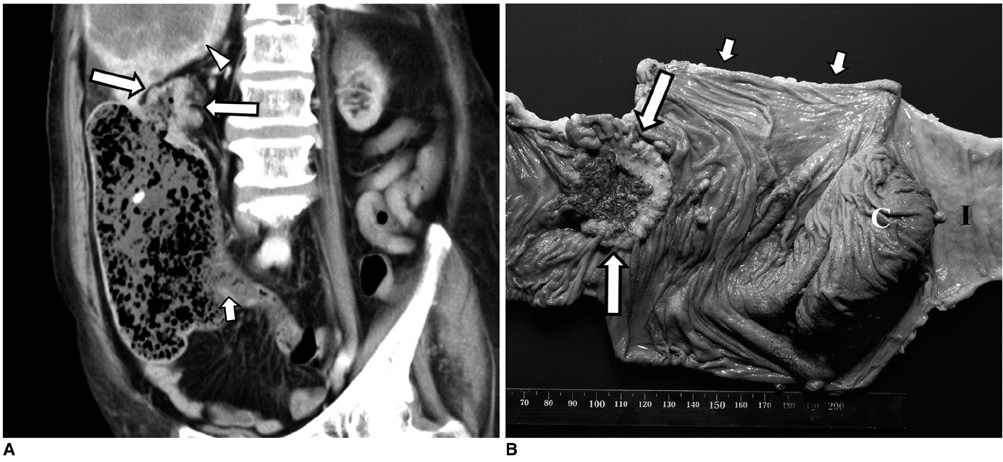
Fig. 2 75-year-old woman with closed-loop obstruction secondary to adenocarcinoma of ascending colon and she had competent ileocecal valve. A. Oblique coronal reformatted CT image shows obstructive mass in distal ascending colon (arrows) and marked dilatation of proximal colon that was filled with fecal material. Small bowel is not dilated and ileocecal valve area is indicated by short arrow. Also noted is hepatic metastasis (arrowhead). B. Two days after CT scan, patient underwent emergency right hemicolectomy for her colon perforation. Photograph of resected specimen shows obstructive mass in ascending colon (arrows) and segmental dilatation of colon proximal to mass (short arrows). Perforation occurred just below colon cancer (not shown). C = cecum, I = terminal ileum.

Fig. 3 53-year-old woman with adenocarcinoma of sigmoid colon. A, B. Contrast-enhanced axial CT scans show segmental wall thickening with contrast enhancement involving sigmoid colon (arrows in A). Anterior colon wall defect (arrowhead) with pericolic enhancing mass (short arrows) is identified. There is large abscess (arrows in B) in cranial direction to enhancing mass. C. Photograph of specimen reveals ulcerofungating mass (arrows) with focal perforation (arrowhead). Pericolic inflammatory mass is also seen (short arrows).

Fig. 4 72-year-old man with adenocarcinoma of ascending colon. A. Contrast-enhanced axial CT scan shows irregular thickening of ascending colon (arrows) and pericolic fat stranding (curved arrow). B. Caudal to colon wall thickening, there are colon wall defect (arrowheads) at level of ileocecal valve and adjacent peritoneal fluid (short arrow). Free perforation was surgically confirmed at proximal portion of colon cancer.
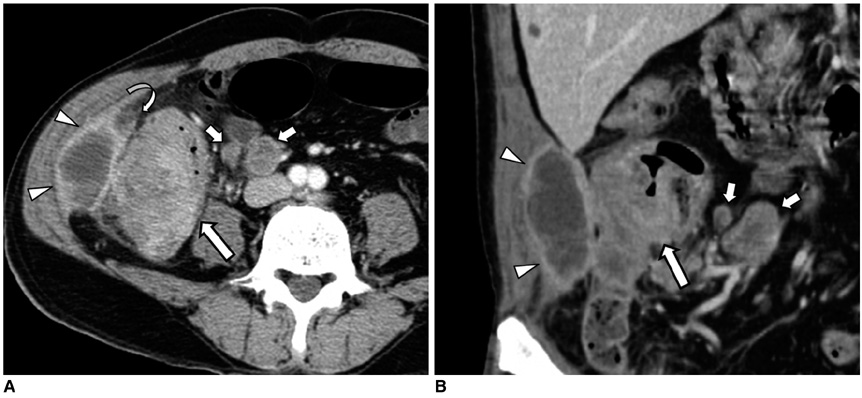
Fig. 5 65-year-old man with adenocarcinoma of ascending colon. A, B. Contrast-enhanced axial CT scan and coronal reformations show colon wall thickening with contrast enhancement (arrows), low-attenuated lesion of right paracolic gutter attached to abdominal wall (arrowheads) and adjacent fat stranding (curved arrow). Note pericolic enlarged lymph nodes (short arrows). Pericolic low-density lesion was surgically confirmed and it was pathologically diagnosed as inflammatory mass with abscess. There was no tumor involvement in peritoneal wall.
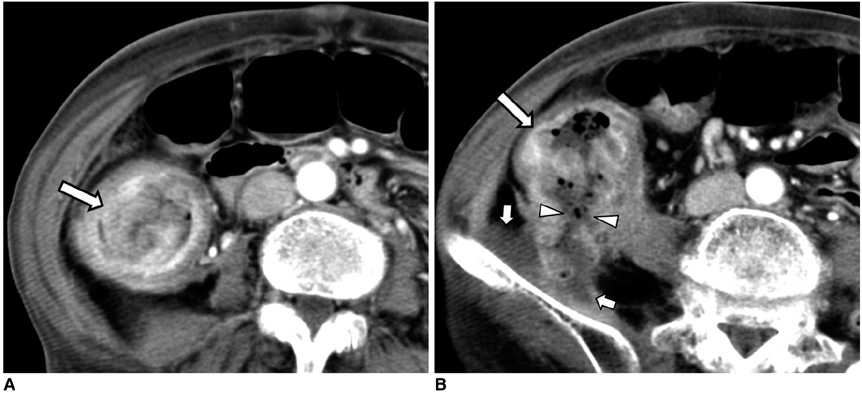
Fig. 6 71-year-old woman with adenocarcinoma of ascending colon. A, B. Contrast-enhanced axial CT scans show polypoid enhancing mass with colon wall thickening (arrows). Colon perforation occurred at posterior wall of ascending colon (arrowheads), resulting in abscess formation in iliacus muscle (short arrows).
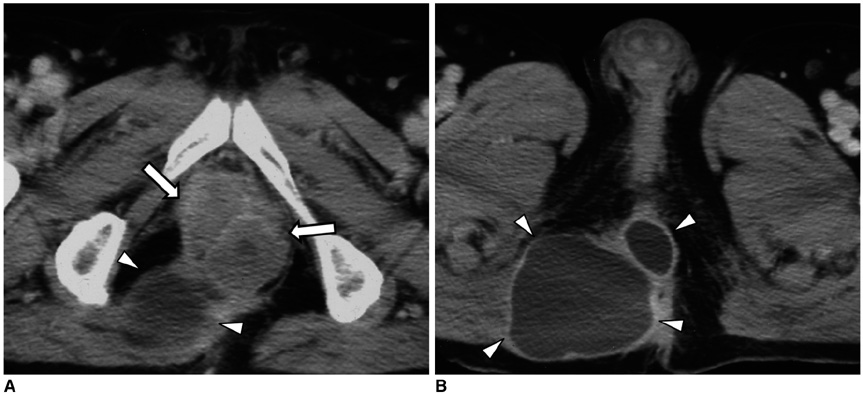
Fig. 7 74-year-old man with adenocarcinoma of rectum. A, B. Contrast-enhanced axial CT scans show irregular, enhancing mass in rectum (arrows) with abscesses in perianal area (arrowheads).
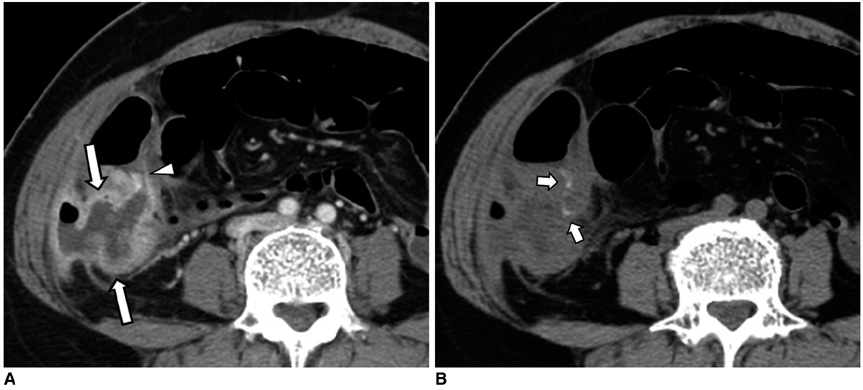
Fig. 8 48-year-old woman with perforated mucinous carcinoma of appendix. A. Contrast-enhanced axial CT scans show irregular, peripheral enhancing low-density lesion (arrows) connected to cecum (arrowhead). This air-containing lesion extends laterally to abdominal wall through retroperitoneum, and it mimics appearance of perforated appendicitis with periappendiceal abscess. B. Nonenhanced axial CT image shows intratumoral calcifications (short arrows). Perforated mucinous carcinoma of appendix with direct invasion into abdominal wall was pathologically confirmed.

Fig. 9 47-year-old man with mucinous adenocarcinoma involving cecum and proximal ascending colon. A, B. Contrast-enhanced axial CT scans show marked circumferential wall thickening with large areas of low attenuation in cecum (arrows). Two lesions with low attenuation are identified in anterior abdominal wall (arrowheads) and pelvic cavity (short arrows), respectively. C. At surgery, thickened colon wall was seen to be adhered to anterior abdominal wall (arrow). Mucinous material was drained from anterior abdominal wall during surgery, indicating that mucinous material spread by direct extension. There was also mucinous material in pelvic cavity. Perforated mucinous adenocarcinoma was pathologically confirmed.
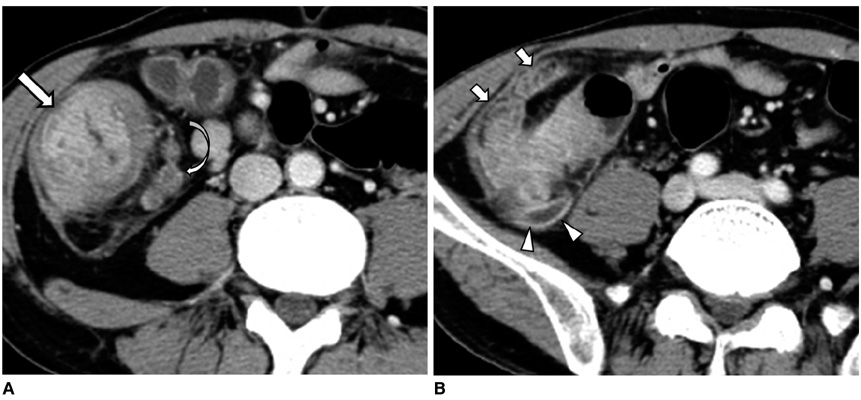
Fig. 10 40-year-old man with cecal adenocarcinoma and he presented with acute pain in right lower quadrant and leukocytosis. A, B. Contrast-enhanced axial CT scans show wall thickening with contrast enhancement in cecum (arrow) and thickened appendix (arrowheads). Surrounding fat stranding is severe (short arrows). Note pericolic enlarged lymph nodes (curved arrow). Cecal adenocarcinoma with invasion of appendix that resulted in acute appendicitis was pathologically confirmed.
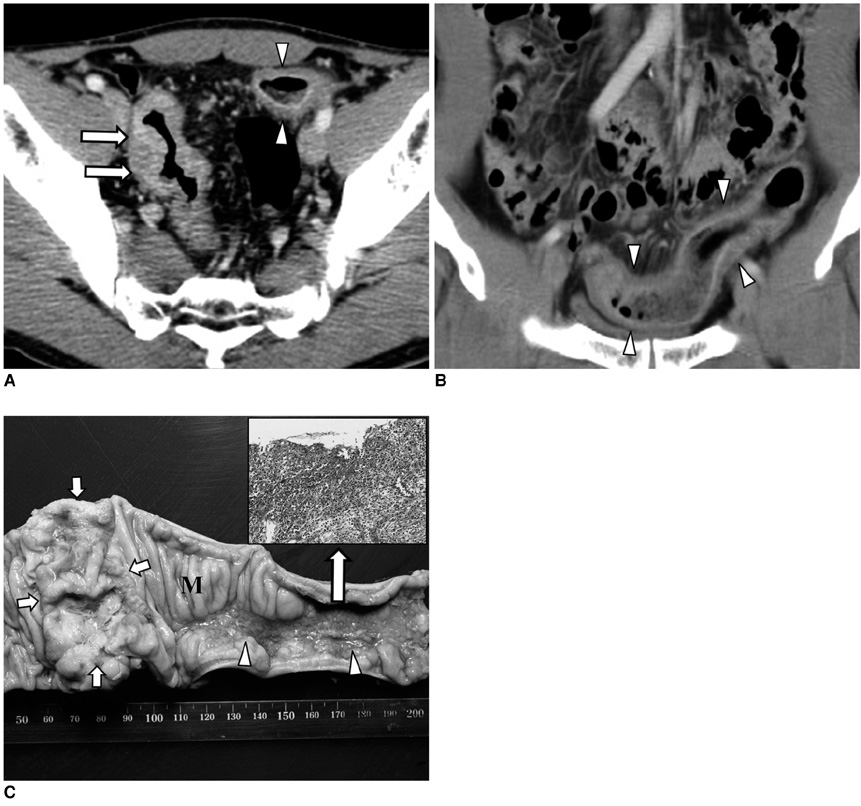
Fig. 11 55-year-old man with ischemic colitis proximal to adenocarcinoma of sigmoid colon. A, B. Contrast-enhanced axial CT scan and coronal reformations show irregular concentric wall thickening of sigmoid colon with contrast enhancement (arrows). Proximal to tumor segment, there is smooth, annular wall thickening with layered enhancement pattern involving long segment of sigmoid colon (arrowheads). C. Photograph of resected specimen shows ulcerofungating mass in sigmoid colon (short arrows) and diffuse mucosal ulceration extending 10 cm proximal to tumor segment (arrowheads). This mucosal lesion was pathologically confirmed to be ischemic colitis (inset). Note intervening normal mucosa (M) between tumor and ischemic segment.
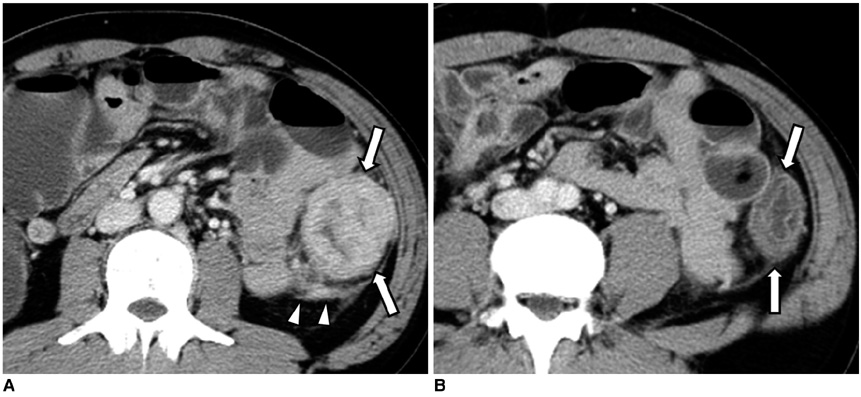
Fig. 12 41-year-old man with adenocarcinoma of descending colon that was accompanied by distal segment of wall edema. A. Contrast-enhanced axial CT scan shows large mass with contrast enhancement involving descending colon (arrows). Also note pericolic infiltration (arrowheads). B. Axial CT scan obtained inferior to A shows mild annular wall thickening with preservation of wall layer in descending colon distal to tumor segment (arrows).

Fig. 13 52-year-old woman with ileocolic intussusception secondary to adenocarcinoma of ascending colon. A. Coronal reformatted CT image shows invagination of ileal loop into colon (arrowheads). B. Coronal reformatted CT image obtained posterior to A shows polypoid mass with contrast enhancement in ascending colon (arrows).

Fig. 14 59-year-old woman with colocolic intussusception secondary to adenocarcinoma of sigmoid colon. A, B. Contrast-enhanced axial CT scan and sagittal reformations show invagination of segment of colon (intussusceptum, arrowheads) through intussuscipiens (arrows). Note that lead point is seen as enhancing mass (M).
Reference
-
1. Horton KM, Abrams RA, Fishman EK. Spiral CT of colon cancer: imaging features and role in management. Radiographics. 2000. 20:419–430.2. Filippone A, Ambrosini R, Fuschi M, Marinelli T, Genovesi D, Bonomo L. Preoperative T and N staging of colorectal cancer: accuracy of contrast-enhanced multi-detector row CT colonography--initial experience. Radiology. 2004. 231:83–90.3. Biondo S, Kreisler E, Millan M, Fraccalvieri D, Golda T, Marti Rague J, et al. Differences in patient postoperative and long-term outcomes between obstructive and perforated colonic cancer. Am J Surg. 2008. 195:427–432.4. Hoeffel C, Crema MD, Belkacem A, Azizi L, Lewin M, Arrive L, et al. Multi-detector row CT: spectrum of diseases involving the ileocecal area. Radiographics. 2006. 26:1373–1390.5. Rovito PF, Verazin G, Prorok JJ. Obstructing carcinoma of the cecum. J Surg Oncol. 1990. 45:177–179.6. Balthazar EJ, Birnbaum BA, Megibow AJ, Gordon RB, Whelan CA, Hulnick DH. Closed-loop and strangulating intestinal obstruction: CT signs. Radiology. 1992. 185:769–775.7. McKay A, Bathe OF. A novel technique to relieve a closed-loop obstruction secondary to a competent ileocecal valve and an unresectable mid-colon tumor. J Gastrointest Surg. 2007. 11:1365–1367.8. Hulnick DH, Megibow AJ, Balthazar EJ, Gordon RB, Surapenini R, Bosniak MA. Perforated colorectal neoplasms: correlation of clinical, contrast enema, and CT examinations. Radiology. 1987. 164:611–615.9. Tsai HL, Hsieh JS, Yu FJ, Wu DC, Chen FM, Huang CJ, et al. Perforated colonic cancer presenting as intra-abdominal abscess. Int J Colorectal Dis. 2007. 22:15–19.10. Kim SH, Shin SS, Jeong YY, Heo SH, Kim JW, Kang HK. Gastrointestinal tract perforation: MDCT findings according to the perforation sites. Korean J Radiol. 2009. 10:63–70.11. Okita A, Kubo Y, Tanada M, Kurita A, Takashima S. Unusual abscesses associated with colon cancer: report of three cases. Acta Med Okayama. 2007. 61:107–113.12. Matsumoto G, Asano H, Kato E, Matsuno S. Transverse colonic cancer presenting as an anterior abdominal wall abscess: report of a case. Surg Today. 2001. 31:166–169.13. Tsukuda K, Ikeda E, Miyake T, Ishihara Y, Watatani H, Nogami T, et al. Abdominal wall and thigh abscess resulting from the penetration of ascending colon cancer. Acta Med Okayama. 2005. 59:281–283.14. Pereira JM, Sirlin CB, Pinto PS, Jeffrey RB, Stella DL, Casola G. Disproportionate fat stranding: a helpful CT sign in patients with acute abdominal pain. Radiographics. 2004. 24:703–715.15. Arjona Sanchez A, Tordera Torres EM, Cecilia Martinez D, Rufian Pena S. Colon cancer presenting as an appendiceal abscess in a young patient. Can J Surg. 2008. 51:E15–E16.16. Rao PM, Rhea JT, Novelline RA, McCabe CJ, Lawrason JN, Berger DL, et al. Helical CT technique for the diagnosis of appendicitis: prospective evaluation of a focused appendix CT examination. Radiology. 1997. 202:139–144.17. Ko GY, Ha HK, Lee HJ, Jeong YK, Kim PN, Lee MG, et al. Usefulness of CT in patients with ischemic colitis proximal to colonic cancer. AJR Am J Roentgenol. 1997. 168:951–956.18. Xiong L, Chintapalli KN, Dodd GD 3rd, Chopra S, Pastrano JA, Hill C, et al. Frequency and CT patterns of bowel wall thickening proximal to cancer of the colon. AJR Am J Roentgenol. 2004. 182:905–909.19. Jang HJ, Lim HK, Park CK, Kim SH, Park JM, Choi YL. Segmental wall thickening in the colonic loop distal to colonic carcinoma at CT: importance and histopathologic correlation. Radiology. 2000. 216:712–717.20. Kim YH, Blake MA, Harisinghani MG, Archer-Arroyo K, Hahn PF, Pitman MB, et al. Adult intestinal intussusception: CT appearances and identification of a causative lead point. Radiographics. 2006. 26:733–744.21. Tresoldi S, Kim YH, Blake MA, Harisinghani MG, Hahn PF, Baker SP, et al. Adult intestinal intussusception: can abdominal MDCT distinguish an intussusception caused by a lead point? Abdom Imaging. 2008. 33:582–588.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Association of Anisakiasis in the Ascending Colon with Sigmoid Colon Cancer: CT Colonography Findings
- Diagnostic Value of Computed Tomography in the Colon Cancer: In Terms of the Staging System
- Imaging Analysis of Colonic Villous Tumors
- CT Findings of Non-specific Colonic Edema in Liver Cirrhosis
- A Case of Inserting Two Self-expandable Metal Stents in Dual Malignant Colonic Obstructions
