Interventional Management of Esophagorespiratory Fistula
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 138-736, Korea. hysong@amc.seoul.kr
- KMID: 1783188
- DOI: http://doi.org/10.3348/kjr.2010.11.2.133
Abstract
- An esophagorespiratory fistula (ERF) is an often fatal consequence of esophageal or bronchogenic carcinomas. The preferred treatment is placement of esophageal and/or airway stents. Stent placement must be performed as quickly as possible since patients with ERFs are at a high risk for aspiration pneumonia. In this review, choice of stents and stenting area, fistula reopening and its management, and the long-term outcome in the interventional management of malignant ERFs are considered. Lastly, a review of esophagopulmonary fistulas will also be provided.
MeSH Terms
Figure
-
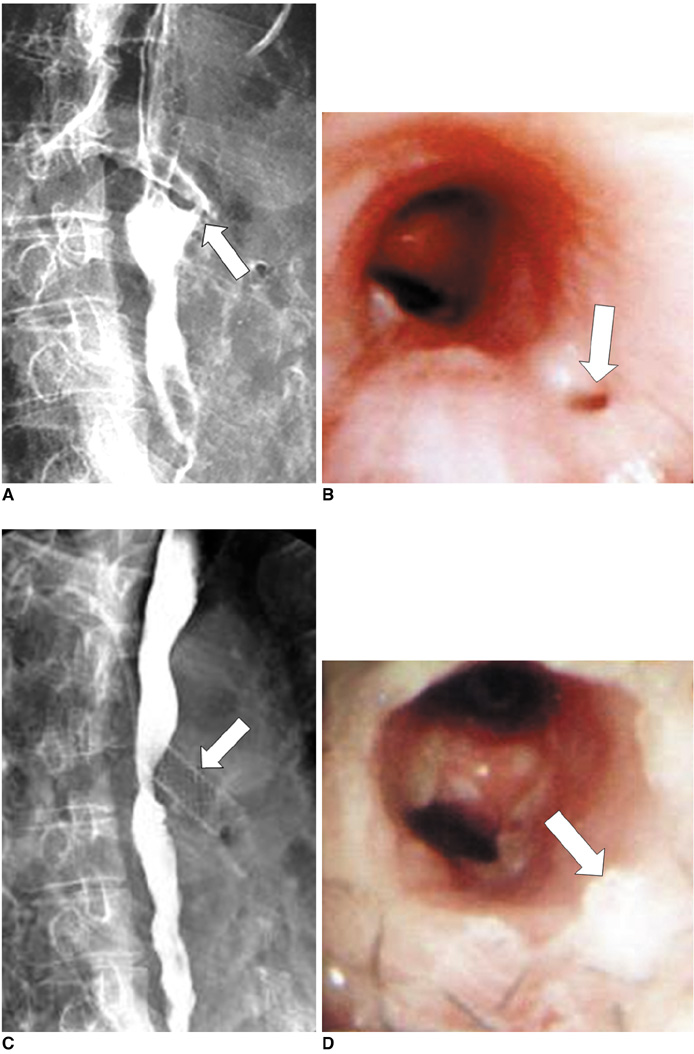
Fig. 1 Esophagobronchial fistula due to pressure necrosis by esophageal stent. Esophagogram (A) and bronchoscopy (B) after esophageal stent removal shows definite fistula (arrows) at proximal end of stent site. Esophagogram (C) and bronchoscopy (D) after bronchial stent placement (arrows), shows successful closure of fistula.
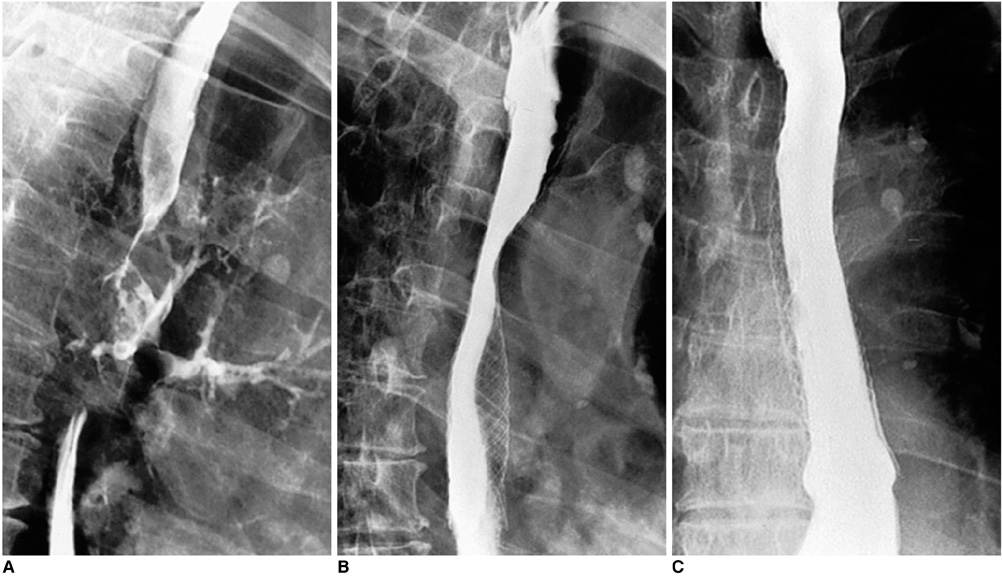
Fig. 2 Esophageal cancer with development of esophagobronchial fistula. Ingested contrast medium is aspirated into left bronchi (A). Right anterior oblique (B) and anteroposterior (C) esophagograms obtained two days after placement of covered expandable metallic stent (18 mm in diameter), shows complete closure of fistula.

Fig. 3 Determination of stenting area in various types of esophagorespiratory fistula. A. Esophageal stenting is indicated when esophageal stricture is severe, but with no or only mild airway stricture. B. Airway stenting is indicated when esophageal and airway strictures are non-existent or mild. C. Airway stenting is indicated when airway stricture is severe, but without or with only mild esophageal stricture. D. Both airway and esophageal stenting is indicated when both esophageal and airway stenosis is severe. M and S denotes mild or severe degree of stenosis, respectively.
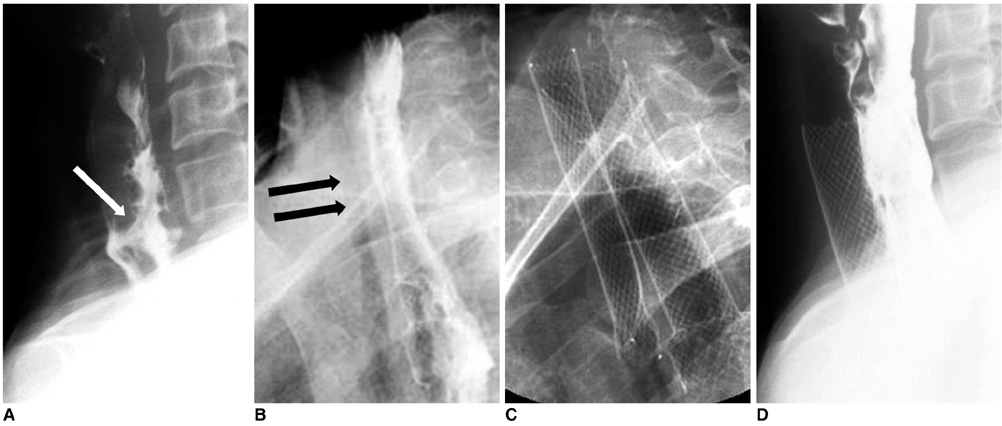
Fig. 4 Esophageal cancer and esophagotracheal fistula. A. Lateral esophagogram shows esophagotracheal fistula (arrow) and segmental luminal narrowing in cervical esophagus. B. Radiograph obtained one week following esophageal stent placement shows diffuse tracheal narrowing (arrows). C. Radiograph obtained following tracheal stent placement to relieve dyspnea. D. Esophagogram obtained one week after tracheal stent placement shows good flow of contrast medium through esophageal stent without visualization of fistula and fully expanded tracheal stent.
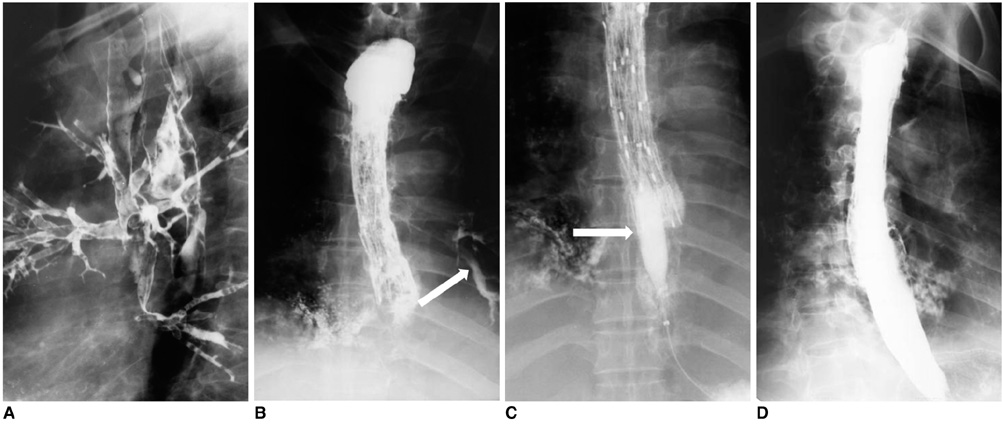
Fig. 5 Reopening of esophagobronchial fistula caused by food impaction. A. Initial lateral view shows fistula caused by esophageal cancer. Subsequently, placement of covered expandable stent was performed. B. Esophagogram obtained one month after stent placement, shows reopening of fistula (arrow) due to food impaction, which is seen as filling defects within stent. C. This patient underwent passage of inflated balloon catheter (arrow) up and down occluded stent to displace impacted food into stomach. D. Esophagogram obtained after cleansing stent, shows stent patency and disappearance of fistula.
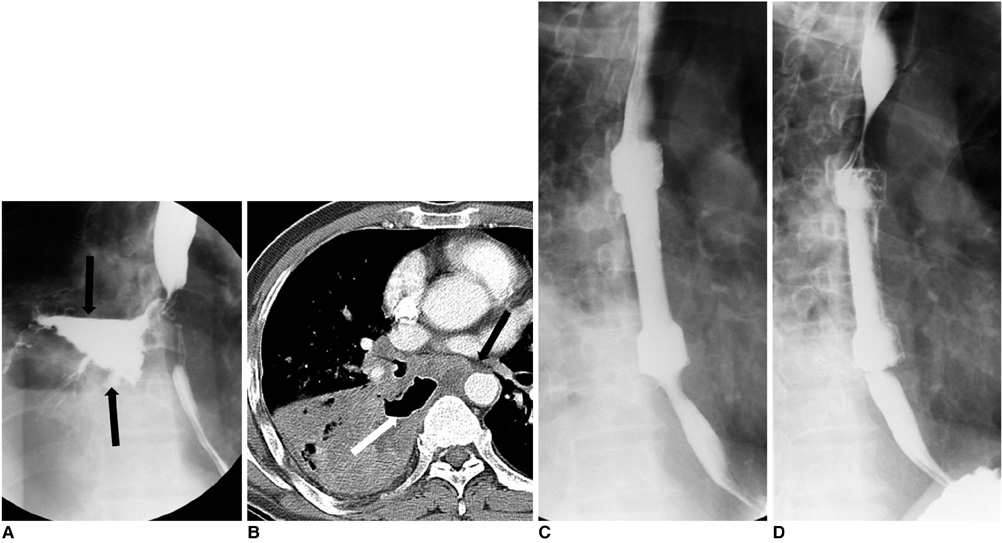
Fig. 6 Esophagopulmonary fistula caused by lung cancer. Esophagogram (A) and CT scan (B) show large lung abscess (arrows) connected to esophagus. Immediate (C) and one-month (D) follow-up esophagograms show successful closure of fistula.
Reference
-
1. Shin JH, Song HY, Ko GY, Lim JO, Yoon HK, Sung KB. Esophagorespiratory fistula: long-term results of palliative treatment with covered expandable metallic stents in 61 patients. Radiology. 2004. 232:252–259.2. Martini N, Goodner JT, D'Angio GJ, Beattie EJ Jr. Tracheoesophageal fistula due to cancer. J Thorac Cardiovasc Surg. 1970. 59:319–324.3. Balazs A, Galambos Z, Kupcsulik PK. Characteristics of esophagorespiratory fistulas resulting from esophageal cancers: a single-center study on 243 cases in a 20-year period. World J Surg. 2009. 33:994–1001.4. Murthy S, Gonzalez-Stawinski GV, Rozas MS, Gildea TR, Dumot JA. Palliation of malignant aerodigestive fistulae with self-expanding metallic stents. Dis Esophagus. 2007. 20:386–389.5. Weigert N, Neuhaus H, Rosch T, Hoffmann W, Dittler HJ, Classen M. Treatment of esophagorespiratory fistulas with silicone-coated self-expanding metal stents. Gastrointest Endosc. 1995. 41:490–496.6. Abadal JM, Echenagusia A, Simo G, Camunez F. Treatment of malignant esophagorespiratory fistulas with covered stents. Abdom Imaging. 2001. 26:565–569.7. Tomaselli F, Maier A, Sankin O, Woltsche M, Pinter H, Smolle-Juttner FM. Successful endoscopical sealing of malignant esophageotracheal fistulae by using a covered self-expandable stenting system. Eur J Cardiothorac Surg. 2001. 20:734–738.8. Han YM, Song HY, Lee JM, Cho SI, Chung GH, Kim CS, et al. Esophagorespiratory fistulae due to esophageal carcinoma: palliation with a covered Gianturco stent. Radiology. 1996. 199:65–70.9. Saxon RR, Barton RE, Katon RM, Petersen BD, Lakin PC, Timmermans H, et al. Treatment of malignant esophageal obstructions with covered metallic Z stents: long-term results in 52 patients. J Vasc Interv Radiol. 1995. 6:747–754.10. Kishi K, Nakao T, Goto H, Kimura M, Sonomura T, Yamanaka N, et al. A fast placement technique for covered tracheobronchial stents in patients with complicated esophagorespiratory fistulas. Cardiovasc Intervent Radiol. 2005. 28:485–489.11. van den Bongard HJ, Boot H, Baas P, Taal BG. The role of parallel stent insertion in patients with esophagorespiratory fistulas. Gastrointest Endosc. 2002. 55:110–115.12. Balazs A, Kupcsulik PK, Galambos Z. Esophagorespiratory fistulas of tumorous origin. Non-operative management of 264 cases in a 20-year period. Eur J Cardiothorac Surg. 2008. 34:1103–1107.13. Seto Y, Yamada K, Fukuda T, Hosoi N, Takebayashi R, Chin K, et al. Esophageal bypass using a gastric tube and a cardiostomy for malignant esophagorespiratory fistula. Am J Surg. 2007. 193:792–793.14. Wang MQ, Sze DY, Wang ZP, Wang ZQ, Gao YA, Dake MD. Delayed complications after esophageal stent placement for treatment of malignant esophageal obstructions and esophagorespiratory fistulas. J Vasc Interv Radiol. 2001. 12:465–474.15. Deviere J, Quarre JP, Love J, Cremer M. Self-expandable stent and injection of tissue adhesive for malignant bronchoesophageal fistula. Gastrointest Endosc. 1994. 40:508–510.16. Saxon RR, Barton RE, Katon RM, Lakin PC, Timmermans HA, Uchida BT, et al. Treatment of malignant esophagorespiratory fistulas with silicone-covered metallic Z stents. J Vasc Interv Radiol. 1995. 6:237–242.17. Nam DH, Shin JH, Song HY, Jung GS, Han YM. Malignant esophageal-tracheobronchial strictures: parallel placement of covered retrievable expandable nitinol stents. Acta Radiol. 2006. 47:3–9.18. Binkert CA, Petersen BD. Two fatal complications after parallel tracheal-esophageal stenting. Cardiovasc Intervent Radiol. 2002. 25:144–147.19. Hu Y, Zhao YF, Chen LQ, Zhu ZJ, Liu LX, Wang Y, et al. Comparative study of different treatments for malignant tracheoesophageal/bronchoesophageal fistulae. Dis Esophagus. 2009. 22:526–531.20. Duranceau A, Jamieson GG. Malignant tracheoesophageal fistula. Ann Thorac Surg. 1984. 37:346–354.21. Angorn IB. Intubation in the treatment of carcinoma of the esophagus. World J Surg. 1981. 5:535–541.22. Kim KR, Shin JH, Song HY, Ko GY, Kim JH, Yoon HK, et al. Palliative treatment of malignant esophagopulmonary fistulas with covered expandable metallic stents. AJR Am J Roentgenol. 2009. 193:W278–W282.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Tuberculous Esophagorespiratory Fistula Managed by Silicone - Covered Self - Expendable Metal Stent
- Treatment of Esophagorespiratory Fistulas with Silicone-Coated Self-Expanding Metal Stents
- Treatment of Esophagorespiratory Fistulas Associated with Esophageal Carcinoma: Effectiveness and Problems of a Modified Gianturco Stent
- Interventional Management of Gastrointestinal Fistulas
- Silicone - Covered Self - Expandable Metal Stents for the Palliation of Malignant Esophageal Obstruction and Esophagorespiratory Fistulas
