Catecholamines May Play an Important Role in the Pathogenesis of Transient Mid- and Basal Ventricular Ballooning Syndrome
- Affiliations
-
- 1Department of Internal Medicine, Chungnam National University Hospital, Daejeon, Korea. jaehpark@cnuh.co.kr
- KMID: 1783080
- DOI: http://doi.org/10.3346/jkms.2008.23.5.898
Abstract
- The exact pathogenesis of transient mid- and basal ventricular ballooning, a new variant of transient left ventricular (LV) ballooning, remains unknown. We report two cases of transient mid- and basal ventricular ballooning associated with catecholamines. These cases suggest that catecholamine-mediated myocardial dysfunction might be a potential mechanism of this syndrome.
MeSH Terms
Figure
-
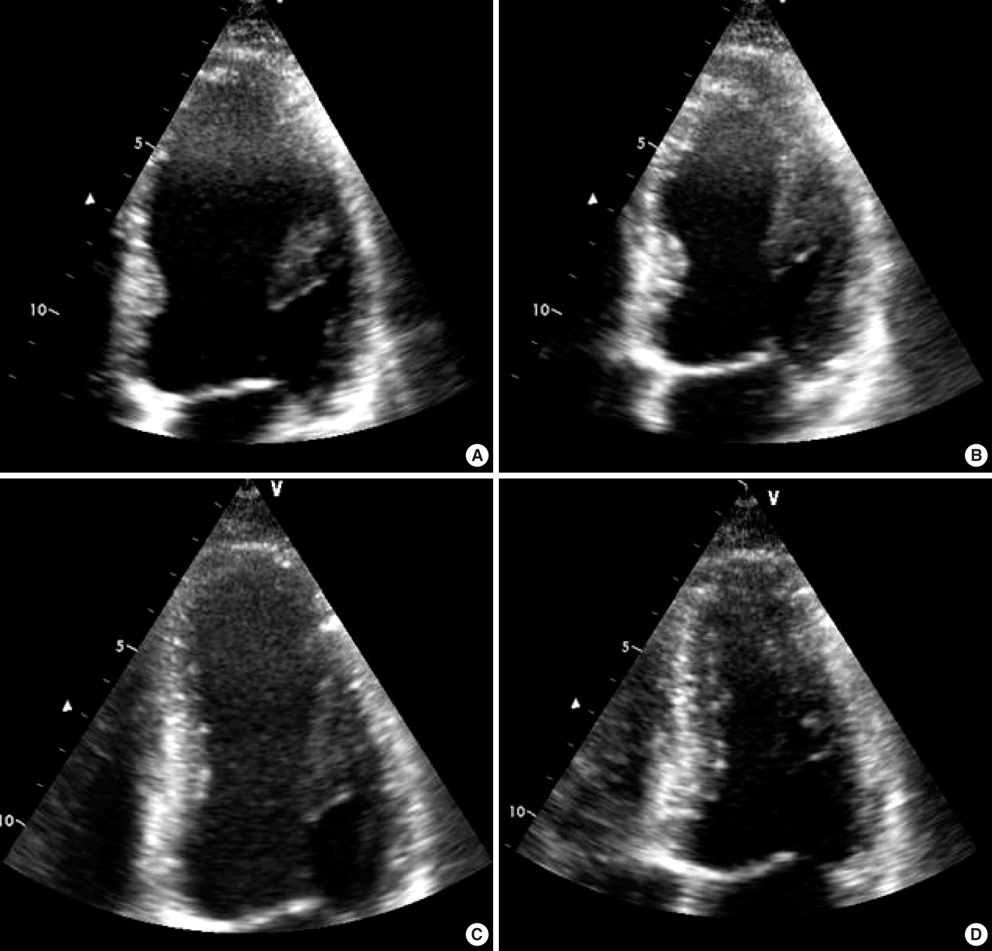
Fig. 1 An apical four-chamber view of the left ventricle in the emergency department is shown at end-diastole (A) and end-systole (B). At end-systole, mid- and basal ventricular ballooning was noted. The follow-up echocardiographic study was performed after three days of treatment. The left ventricular dimension was decreased and ballooning had disappeared (C at end-diastole and D at end-systole).
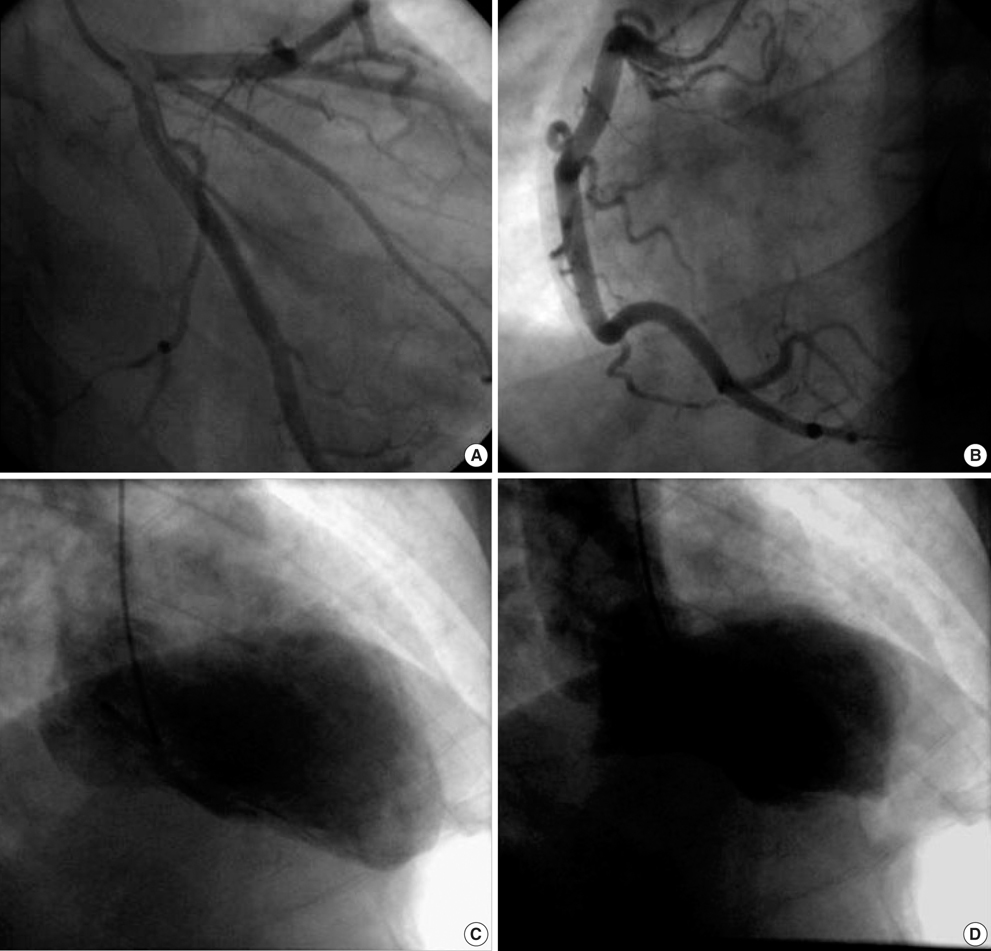
Fig. 2 The coronary angiogram showed normal left (A) and right coronary arteries (B). The left ventriculogram in the right anterior oblique view showed at end-diastole (C) and end-systole (D). At end-systole, mid- and basal ventricular ballooning was noted. However, LV apical motion was normal.
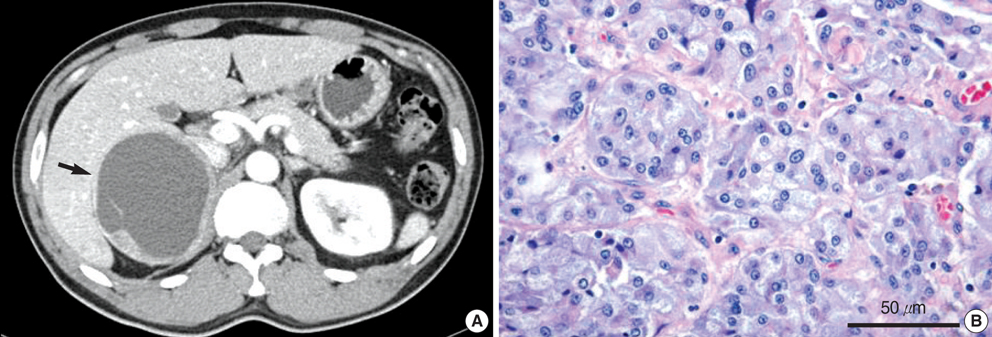
Fig. 3 (A) Abdominal computerized tomography showed an approximately 7.8×8.3×10.0 cm sized large septated cystic mass with irregular wall enhancement of the right adrenal gland (arrow). (B) Large and pink cells are arranged in nests with capillaries between them in the high power field image, which is compatible with pheochromocytoma.
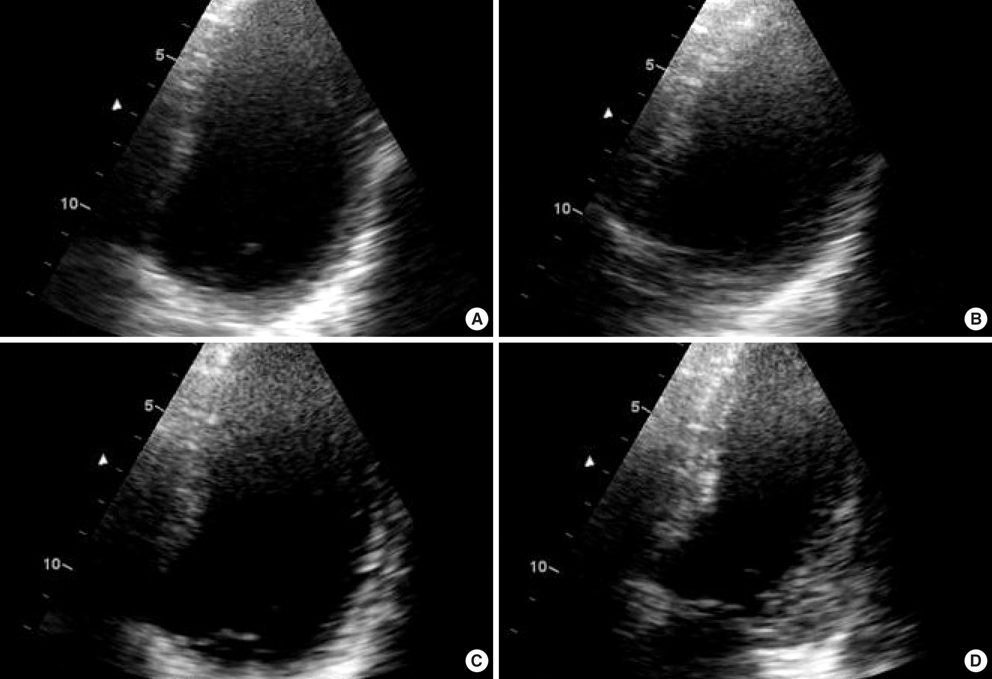
Fig. 4 An apical four-chamber view of the left ventricle after operation is shown at end-diastole (A) and end-systole (B). At end-systole, the mid-and basal ventricular ballooning was noted with sparing of the LV apex. A follow-up echocardiographic study was performed after two days. The left ventricular dimension had decreased and ballooning was no longer present (C at end-diastole and D at end-systole).
Cited by 2 articles
-
A Case of Acute ST-Segment Elevation Myocardial Infarction Mimicking Stress Induced Cardiomyopathy; Demonstration of Typical Echocardiographic Finding Correlated with Unusual Distribution of Left Anterior Descending Coronary Artery
Sung Kyun Shin, Seon-Ah Jin, Yong Kyu Park, Jae-Hyeong Park
J Cardiovasc Ultrasound. 2010;18(3):101-103. doi: 10.4250/jcu.2010.18.3.101.Prevalence and Patterns of Left Ventricular Dysfunction in Patients with Pheochromocytoma
Jae-Hyeong Park, Kyu Seop Kim, Ji-Young Sul, Sung Kyun Shin, Jun Hyung Kim, Jae-Hwan Lee, Si Wan Choi, Jin-Ok Jeong, In-Whan Seong
J Cardiovasc Ultrasound. 2011;19(2):76-82. doi: 10.4250/jcu.2011.19.2.76.
Reference
-
1. Hurst RT, Askew JW, Reuss CS, Lee RW, Sweeney JP, Fortuin FD, Oh JK, Tajik AJ. Transient midventricular ballooning syndrome: a new variant. J Am Coll Cardiol. 2006. 48:579–583.2. Yasu T, Tone K, Kubo N, Saito M. Transient mid-ventricular ballooning cardiomyopathy: a new entity of Takotsubo cardiomyopathy. Int J Cardiol. 2006. 110:100–101.
Article3. Tsuchihashi K, Ueshima K, Uchida T, Oh-mura N, Kimura K, Owa M, Yoshiyama M, Miyazaki S, Haze K, Ogawa H, Honda T, Hase M, Kai R, Morii I. Angina Pectoris-Myocardial Infarction Investigations in Japan. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. Angina Pectoris-Myocardial Infarction Investigations in Japan. J Am Coll Cardiol. 2001. 38:11–18.4. Park JH, Kang SJ, Song JK, Kim HK, Lim CM, Kang DH, Koh Y. Left ventricular apical ballooning due to severe physical stress in patients admitted to the medical ICU. Chest. 2005. 128:296–302.
Article5. Wittstein IS, Thiemann DR, Lima JA, Baughman KL, Schulman SP, Gerstenblith G, Wu KC, Rade JJ, Bivalacqua TJ, Champion HC. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005. 352:539–548.
Article6. Lacy CR, Contrada RJ, Robbins ML, Tannenbaum AK, Moreyra AE, Chelton S, Kostis JB. Coronary vasoconstriction induced by mental stress (simulated public speaking). Am J Cardiol. 1995. 75:503–505.
Article7. Bolli R, Marban E. Molecular and cellular mechanisms of myocardial stunning. Physiol Rev. 1999. 79:609–634.
Article8. Takizawa M, Kobayakawa N, Uozumi H, Yonemura S, Kodama T, Fukusima K, Takeuchi H, Kaneko Y, Kaneko T, Fujita K, Honma Y, Aoyagi T. A case of transient left ventricular ballooning with pheochromocytoma, supporting pathogenetic role of catecholamines in stress-induced cardiomyopathy or takotsubo cardiomyopathy. Int J Cardiol. 2007. 114:e15–e17.
Article9. Pierpont GL, DeMaster EG, Cohn JN. Regional differences in adrenergic function within the left ventricle. Am J Physiol. 1984. 246:H824–H829.
Article10. Kawano H, Okada R, Yano K. Histological study on the distribution of autonomic nerves in the human heart. Heart Vessels. 2003. 18:32–39.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of transient mid-ventricular ballooning syndrome
- A case of stress-induced cardiomyopathy with an "inverted Takotsubo" contractile pattern
- A Case of Transient Mid-Ventricular Ballooning Syndrome after Cardiac Arrest
- A Case of Malignant Pheochromocytoma Presenting as Inverted Takotsubo-Like Cardiomyopathy
- Magnetic Resonance Imaging of Transient Left Ventricular Apical Ballooning Related to Emotional Stress: a Case Report
