Implantable Cardioverter-Defibrillator Implantation in a Patient with Atrial Standstill
- Affiliations
-
- 1Department of Internal Medicine, Gyeongsang National University College of Medicine, Jinju, Korea. cwakch@korea.com
- KMID: 1782983
- DOI: http://doi.org/10.3349/ymj.2009.50.1.156
Abstract
- We report a 55-year-old female patient who presented with no P waves but with a wide QRS complex escape rhythm at 44 beats/min and prolonged QTc of 0.55 seconds on ECG. The patient had recurrence of ventricular fibrillations and loss of consciousness, and underwent defibrillation and cardiopulmonary resuscitation (CPR) several times because of cardiac arrest. The transthoracic echocardiography showed dilated cardiomyopathy and enlargement of both atria. The Doppler echocardiography documented the absence of A wave in the tricuspid and mitral valve flow. An electrophysiologic study demonstrated electrical inactivity in the right and left atria. Atrial pacing with maximum output did not capture the atria. These findings together with her electrocardiographic finding indicated atrial standstill. Sudden cardiac death was her first clinical manifestation of ventricular arrhythmia. The patient remained asymptomatic after receiving a single chamber implantable cardioverter-defibrillator (ICD) with VVI pacemaker function.
Keyword
MeSH Terms
Figure
-

Fig. 1 Twelve-lead ECG and intracardiac electrogram. (A) Twelve-lead ECG on the 1st day of admission showed an escape distal rhythm at 44 beats/min with wide QRS complex, of 0.12 sec. No P wave was found in ECG. QTc interval was prolonged to 0.55 sec. (B) Recording obtained during EPS after implantation of ICD with VVI pacemaker function. There was no electrical activity on atrial and CS electrograms. ECG, electrocardiogram; ICD, implantable cardioverter-defibrillator; HRA, high right atrium, CS, coronary sinus.
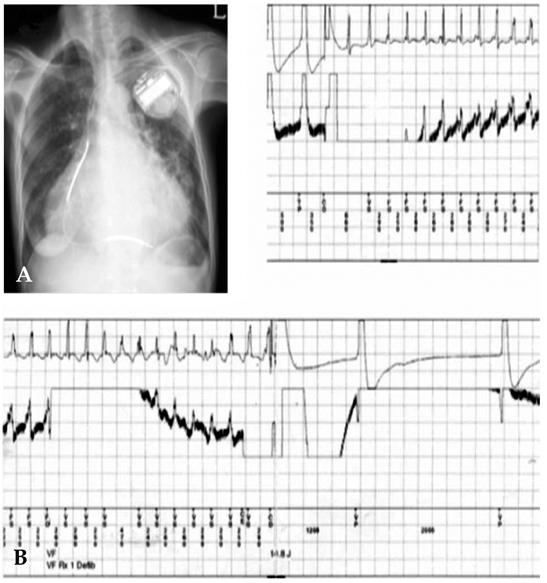
Fig. 2 (A) Chest PA of a single chamber ICD with VVI pacemaker function implanted to the patient. (B) DFT test showed induction of VF, and safe and successful defibrillation at 14.8 J. PA, postero-anterior; ICD, implantable cardioverter-defibrillator; DFT, defibrillation threshold test; VF, ventricular fibrillation.
Cited by 1 articles
-
Fever-Induced QTc Prolongation and Ventricular Fibrillation in a Healthy Young Man
Sun Min Lim, Hui-Nam Pak, Moon-Hyoung Lee, Sung Soon Kim, Boyoung Joung
Yonsei Med J. 2011;52(6):1025-1027. doi: 10.3349/ymj.2011.52.6.1025.
Reference
-
1. Fazelifar AF, Arya A, Haghjoo M, Sadr-Ameli MA. Familial atrial standstill in association with dilated cardiomyopathy. Pacing Clin Electrophysiol. 2005. 28:1005–1008.
Article2. Bensaid J. Persistent atrial standstill documented over a 22-year period. Am Heart J. 1996. 131:404–407.
Article3. Marini M, Arbustini E, Disertori M. Atrial standstill: a paralysis of cardiological relevance. Ital Heart J Suppl. 2004. 5:681–686.4. Bloomfield DA, Sinclair-Smith BC. Persistent atrial standstill. Am J Med. 1965. 39:335–340.
Article5. Rosenbaum FF, Levine SA. Auricular standstill. Its occurrence and significance. Am J Med Sci. 1939. 198:774.6. Koshimizu TA, Komori S, Ishihara T, Kohno I, Umetani K, Sawanobori T, et al. Restored atrial excitability after late recanalization in a patient with atrial standstill and acute myocardial infarction. Pacing Clin Electrophysiol. 2002. 25:217–219.7. Groenewegen WA, Firouzi M, Bezzina CR, Vliex S, van Langen IM, Sandkuijl L, et al. A cardiac sodium channel mutation cosegregates with a rare connexin 40 genotype in familial atrial standstill. Circ Res. 2003. 92:14–22.
Article8. Shaw TR, Northridge DB, Francis CM. Left atrial standstill in a patient with mitral stenosis and sinus rhythm: a risk of thrombus hidden by left and right atrial electrical dissociation. Heart. 2003. 89:1173.
Article9. Bhuiyan ZA, van den Berg MP, van Tintelen JP, Bink-Boelkens MT, Wiesfeld AC, Alders M, et al. Expanding spectrum of human RYR2-related disease: new electrocardiographic, structural, and genetic features. Circulation. 2007. 116:1569–1576.10. Rosen KM, Rahimtoola SH, Gunnar RM, Lev M. Transient and persistent atrial standstill with His bundle lesions. Electrophysiologic and pathologic correlations. Circulation. 1971. 44:220–236.
Article11. Nakazato Y, Nakata Y, Hisaoka T, Sumiyoshi M, Ogura S, Yamaguchi H. Clinical and electrophysiological characteristics of atrial standstill. Pacing Clin Electrophysiol. 1995. 18:1244–1254.
Article12. Williams DO, Jones EL, Nagle RE, Smith BS. Familial atrial cardiomyopathy with heart block. Q J Med. 1972. 41:491–508.13. Amat-y-Leon F, Racki AJ, Denes P, Ten Eick RE, Singer DH, Bharati S, et al. Familial atrial dysrhythmia with A-V block: Intracellular microelectrode, clinical electrophysiologic, and morphologic observations. Circulation. 1974. 50:1097–1104.14. Jeong MH, Ahn YK, Gill GC, Park JH, Cho JG, Park JC, et al. Tsutsugamushi myocarditis with congestive heart failure and persistent atrial standstill. Jpn Circ J. 1996. 60:382–388.
Article15. Talwar KK, Radhakrishnan S, Chopra P. Myocarditis manifesting as persistent atrial standstill. Int J Cardiol. 1988. 20:283–286.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transvenous Implantation of an Implantable Cardioverter Defibrillator in a Patient Who Had Undergone Tricuspid Valve Replacement
- Implantable Cardioverter-Defibrillator (ICD) Therapy: Initial Clinical Experience in 6 Patients
- A Case Report of the Patient Implanted with Automatic Implantable Cardioverter Defibrillator (AICD) Subject to 3rd Molar Extraction using Target Controlled Infusion of Propofol and Remifentanil: A Case Report
- Combined Subpectoral Implantation of Implantable Cardioverter-Defibrillator and Augmentation Mammoplasty in a Young Female Patient
- Delayed Perforation of the Right Ventricular Wall by a Single Standard-Caliber Implantable Cardioverter-Defibrillator Lead Detected by Multidetector Computed Tomography
