Yonsei Med J.
2008 Dec;49(6):1055-1059. 10.3349/ymj.2008.49.6.1055.
A Case of Acute Hepatitis with Mycoplasma pneumoniae Infection and Transient Depression of Multiple Coagulation Factors
- Affiliations
-
- 1Department of Pediatrics, Inha University College of Medicine, Incheon, Korea. hee715@freechal.com
- 2Department of Pathology, Inha University College of Medicine, Incheon, Korea.
- KMID: 1782959
- DOI: http://doi.org/10.3349/ymj.2008.49.6.1055
Abstract
- We report a case of acute severe hepatitis with Mycoplasma pneumoniae (M. pneumoniae) infection and transient depression of multiple coagulation factors. A 5-year-old boy, previously healthy, was admitted with pneumonia. M. pneumoniae infection was confirmed by serology testing. Liver enzymes were elevated on admission without any past medical history. After treatment with azithromycin for 3 days, pneumonia improved, but the hepatitis was acutely aggravated. Partial thromboplastin time (PTT) was prolonged and depression of multiple coagulation factors developed. Liver biopsy revealed features consistent with acute hepatitis. A week later, liver enzymes were nearly normalized spontaneously. Normalization of prolonged PTT and coagulation factors were also observed several months later. This may be the first case of transient depression of multiple coagulation factors associated with M. pneumoniae infection.
MeSH Terms
Figure
-
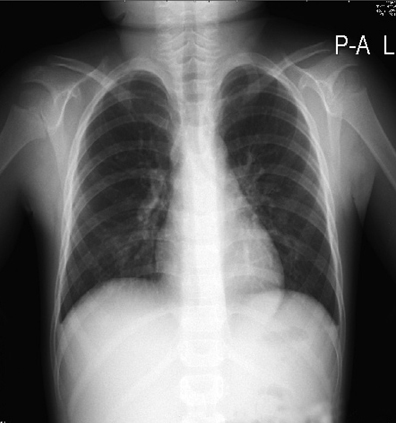
Fig. 1 Chest X-ray shows increased bronchial wall thickening and diffuse infiltration on both lungs.
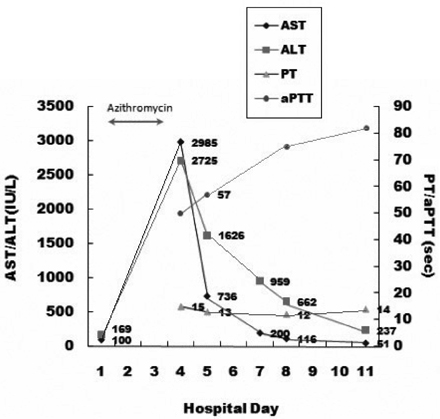
Fig. 2 Progression of the disease.
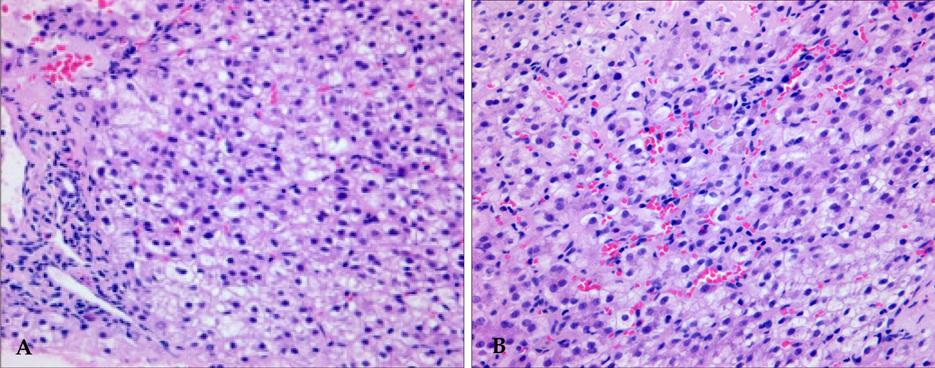
Fig. 3 The portal area (A) and hepatic lobule (B) show features of acute hepatitis such as ballooning degeneration, spotty necrosis and increased Kupffer cell activity (H & E, × 400).
Reference
-
1. Waites KB. New concepts of Mycoplasma pneumoniae infections in children. Pediatr Pulmonol. 2003. 36:267–278.2. Eun BW, Kim NH, Choi EH, Lee HJ. Mycoplasma pneumoniae in Korean children: the epidemiology of pneumonia over 18-year period. J Infect. 2008. 56:326–331.
Article3. Kim JH, Chae SA, Lee DK. Clinical findings of Mycoplasma pneumonia in children, from 1998 to 2003. Korean J Pediatr. 2005. 48:969–975.4. Lee JK, Hong CH, Sohn YM, Kim KE, Kim DH, Kim PK, et al. Mycoplasmal pneumonia in children. Yonsei Med J. 1986. 27:300–306.
Article5. Cherry JD, Ching N. Feigin RD, Cherry JD, editors. Mycoplasma pneumoniae. Textbook of Pediatric Infectious Diseases. 2004. 5th ed. Philadelphia: W.B. Saunders;2516–2531.6. Horii Y, Sugimoto T, Sakamoto I, Sawada T. Acute acalculous cholecystitis complicating Mycoplasma pneumoniae infection. Clin Pediatr (Phila). 1992. 31:376–378.
Article7. Lee YS, Hong CH, Lee C, Lee SG. Unusual forms of pulmonary and extrapulmonary manifestations of mycoplasmal pneumonia. Korean J Pediatr. 1989. 32:1064–1073.8. Suzuyama Y, Iwasaki H, Izumikawa K, Hara K. Clinical complications of Mycoplasma pneumoniae disease: other organs. Yale J Biol Med. 1983. 56:487–491.9. Arav-Boger R, Assia A, Spirer Z, Bujanover Y, Reif S. Cholestatic hepatitis as a main manifestation of Mycoplasma pneumoniae infection. J Pediatr Gastroenterol Nutr. 1995. 21:459–460.
Article10. Grüllich C, Baumert TF, Blum HE. Acute Mycoplasma pneumoniae infection presenting as cholestatic hepatitis. J Clin Microbiol. 2003. 41:514–515.
Article11. Lee JT, Kim HS, Tchah H. Hepatitis complicated with Mycoplasma pneumoniae infection. Korean J Pediatr Gastroenterol Nutr. 2001. 4:207–212.
Article12. Kountouras D, Deutsch M, Emmanuel T, Georgiadis G, Koskinas J. Fulminant Mycoplasma pneumoniae infection with multi-organ involvement: a case report. Eur J Intern Med. 2003. 14:329–331.
Article13. Fernald GW. Immunologic mechanisms suggested in the association of M. pneumoniae infection and extrapulmonary disease: a review. Yale J Biol Med. 1983. 56:475–479.14. Jansson E, Wegelius R, Visakorpi JK. Chronic active hepatitis and concomitant mycoplasma infection. Lancet. 1972. 1:1395.
Article15. Principi N, Esposito S. Comparative tolerability of erythromycin and newer macrolide antibacterials in paediatric patients. Drug Saf. 1999. 20:25–41.
Article16. Fox JC, Szyjkowski RS, Sanderson SO, Levine RA. Progressive cholestatic liver disease associated with clarithromycin treatment. J Clin Pharmacol. 2002. 42:676–680.
Article17. Chandrupatla S, Demetris AJ, Rabinovitz M. Azithromycin-induced intrahepatic cholestasis. Dig Dis Sci. 2002. 47:2186–2188.18. Baciewicz AM, Al-Nimr A, Whelan P. Azithromycin-induced hepatoxicity. Am J Med. 2005. 118:1438–1439.
Article19. Collazos J, Egurbide MV, Atucha K, Esteban P, de Miguel J. Transient acquired factor II deficiency with Mycoplasma pneumoniae infection. J Infect Dis. 1991. 164:434–435.
Article20. Kim MS, Kilgore PE, Kang JS, Kim SY, Lee DY, Kim JS, et al. Transient acquired hemophilia associated with Mycoplasma pneumoniae pneumonia. J Korean Med Sci. 2008. 23:138–141.
Article21. Peuscher FW, van Aken WG, van Mourik JA, Swaak AJ, Sie LH, Statius van Eps LW. Acquired, transient factor X (Stuart factor) deficiency in patient with mycoplasma pneumonial infection. Scand J Haematol. 1979. 23:257–264.22. Levine DP, Lerner AM. The critical spectrum of Mycoplasma pneumoniae infections. Med Clin North Am. 1978. 62:961–978.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case Report of Acute Pancreatitis Caused by Mycoplasma Pneumoniae Infection
- Mycoplasma pneumoniae hepatitis in children
- A Case of Erythema Multiforme in Adults Associated with Mycoplasma pneumoniae Infection
- Mycoplasma pneumoniae-associated Hepatitis without Lung Involvement
- Mycoplasma pneumoniae Infection Presented with Multiple Neurological Complications
