Yonsei Med J.
2008 Dec;49(6):955-964. 10.3349/ymj.2008.49.6.955.
Comparison of Combination Posterior Sub-Tenon Triamcinolone and Modified Grid Laser Treatment with Intravitreal Triamcinolone Treatment in Patients with Diffuse Diabetic Macular Edema
- Affiliations
-
- 1Department of Ophthalmology, NHIC Ilsan Hospital, Gyounggi-do, Korea. hjkoh@yuhs.ac
- 2The Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea.
- 3Jacobs Retina Center at Shiley Eye Center, University of California, San Diego, USA.
- 4Statistical Consultation and Research Center, Department of Preventive Medicine, Keck School of Medicine, University of California, Los Angeles, California, USA.
- 5Yonsei Eye Clinic, Daejeon, Korea.
- KMID: 1782944
- DOI: http://doi.org/10.3349/ymj.2008.49.6.955
Abstract
- PURPOSE
To compare the efficacy of posterior sub-Tenon's capsule triamcinolone acetonide injection combined with modified grid macular photocoagulation (PSTI + MP) with intravitreal triamcinolone acetonide (IVTA) injection in the treatment of diffuse diabetic macular edema (DME). MATERIALS AND METHODS: Forty eyes of 33 patients with diffuse DME were randomly allocated into either PSTI + MP (20 eyes) or IVTA (20 eyes). Best corrected visual acuity (VA) and foveal thickness were measured. RESULTS: The ETDRS scores at baseline were 25.2 +/- 13.6 (mean +/- SD) letters in the PSTI + MP group, whereas 21.7 +/- 16.3 letters in the IVTA group. The ETDRS scores improved by 33.2 +/- 15.9, 34.7 +/- 16.6 and 30.9 +/- 19.0 letters in the PSTI + MP group whereas by 30.9 +/- 15.4, 30.1 +/- 17.9 and 31.5 +/- 15.0 letters in the IVTA group at 1, 3, and 6 months after the treatments, respectively. The VA improved significantly at 1 month and 3 months after both treatments (all p < 0.02, paired t-test). The VA improvements were no longer significant at 6 months in either group. There were no statistically significant differences at any time points between the 2 groups (all p > 0.05, Student's t-test). The foveal thicknesses at baseline and 1, 3, and 6 months after the treatments were 382.8 +/- 148.3, 309.1 +/- 131.3, 319.3 +/- 93.3, 340.4 +/- 123.5micrometer (mean +/- SD) in the PSTI + MP group vs. 369.1 +/- 123.1, 241.4 +/- 52.3, 277.5 +/- 137.4, 290.2 +/- 127.9micrometer in the IVTA group, respectively. Pairwise comparisons revealed significant decrease in foveal thickness at 1 month (p = 0.01, paired t-test) for the PSTI + MP group, and at both 1 month (p < 0.001) and 3 months (p = 0.016) for the IVTA group. There were no statistically significant differences at any time points between the 2 groups (all p > 0.05, Student's t-test). In contrast to the PSTI + MP group, where no complications were noted, the elevation of intra-ocular pressure in 3 of 20 eyes (15%) and a significant increase in average cataract grading were observed in the IVTA group. CONCLUSION: PSTI + MP treatment provides significant improvement of vision in patients with diffuse DME over 3 months, and achieves outcomes comparable to those after IVTA treatment, however, with fewer complications.
Keyword
MeSH Terms
-
Adult
Aged
Anti-Inflammatory Agents/administration & dosage
Diabetic Retinopathy/*drug therapy/physiopathology/*surgery
Female
Fovea Centralis/pathology
Humans
*Laser Coagulation
Macular Edema/complications/*drug therapy/physiopathology/*surgery
Male
Middle Aged
Prospective Studies
Triamcinolone/*administration & dosage
Visual Acuity
Vitreous Body
Figure
-

Fig. 1 Changes in mean ETDRS scores after treatments. ETDRS, Early Treatment Diabetic Retinopathy Study. PSTI, posterior subtenon triamcinolone injection; IVTA, intravitreal triamcinolone acetonide injection; ETDRS, Early Treatment of Diabetic Retinopathy Study
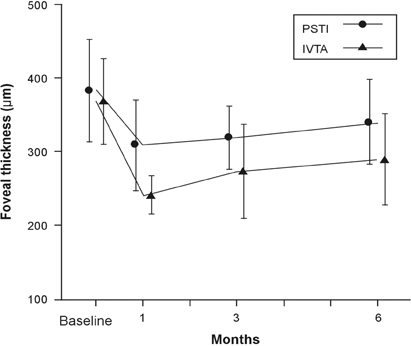
Fig. 2 Changes in mean foveal thicknesses after treatments. PSTI, posterior subtenon triamcinolone injection; IVTA, intravitreal triamcinolone acetonide injection.

Fig. 3 Changes in mean intraocular pressures after treatments. IOP, intraocular pressure; PSTI, posterior subtenon triamcinolone injection; IVTA, intravitreal triamcinolone acetonide injection. *IOP was significantly higher in the IVTA group (p = 0.006 at 1 month, p = 0.026 at 3 months; Student's t-test).
Reference
-
1. Klein R, Klein BE, Moss SE. Visual impairment in diabetes. Ophthalmology. 1984. 91:1–9.2. Focal photocoagulation treatment of diabetic macular edema. Relationship of treatment effect to fluorescein angiographic and other retinal characteristics at baseline: ETDRS report no. 19. Early Treatment Diabetic Retinopathy Study Research Group. Arch Ophthalmol. 1995. 113. 1144–1155.3. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Early Treatment Diabetic Retinopathy Study research group. Arch Ophthalmol. 1985. 103:1796–1806.4. Treatment techniques and clinical guidelines for photocoagulation of diabetic macular edema. Early Treatment Diabetic Retinopathy Study Report Number 2. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. 1987. 94:761–774.5. Martidis A, Duker JS, Greenberg PB, Rogers AH, Puliafito CA, Reichel E, et al. Intravitreal triamcinolone for refractory diabetic macular edema. Ophthalmology. 2002. 109:920–927.
Article6. Massin P, Audren F, Haouchine B, Erginay A, Bergmann JF, Benosman R, et al. Intravitreal triamcinolone acetonide for diabetic diffuse macular edema: preliminary results of a prospective controlled trial. Ophthalmology. 2004. 111:218–224. discussion 224-5.
Article7. Jonas JB, Kreissig I, Söfker A, Degenring RF. Intravitreal injection of triamcinolone for diffuse diabetic macular edema. Arch Ophthalmol. 2003. 121:57–61.
Article8. Sutter FK, Simpson JM, Gillies MC. Intravitreal triamcinolone for diabetic macular edema that persists after laser treatment: three-month efficacy and safety results of a prospective, randomized, double-masked, placebo-controlled clinical trial. Ophthalmology. 2004. 111:2044–2049.
Article9. Entezari M, Ahmadieh H, Dehghan MH, Ramezani A, Bassirnia N, Anissian A. Posterior sub-tenon triamcinolone for refractory diabetic macular edema: a randomized clinical trial. Eur J Ophthalmol. 2005. 15:746–750.
Article10. Verma LK, Vivek MB, Kumar A, Tewari HK, Venkatesh P. A prospective controlled trial to evaluate the adjunctive role of posterior subtenon triamcinolone in the treatment of diffuse diabetic macular edema. J Ocul Pharmacol Ther. 2004. 20:277–284.
Article11. Ohguro N, Okada AA, Tano Y. Trans-Tenon's retrobulbar triamcinolone infusion for diffuse diabetic macular edema. Graefes Arch Clin Exp Ophthalmol. 2004. 242:444–445.12. Bakri SJ, Kaiser PK. Posterior subtenon triamcinolone acetonide for refractory diabetic macular edema. Am J Ophthalmol. 2005. 139:290–294.13. Tunc M, Onder HI, Kaya M. Posterior sub-Tenon's capsule triamcinolone injection combined with focal laser photocoagulation for diabetic macular edema. Ophthalmology. 2005. 112:1086–1091.14. Bonini-Filho MA, Jorge R, Barbosa JC, Calucci D, Cardillo JA, Costa RA. Intravitreal injection versus sub-Tenon's infusion of triamcinolone acetonide for refractory diabetic macular edema: a randomized clinical trial. Invest Ophthalmol Vis Sci. 2005. 46:3845–3849.
Article15. Cellini M, Pazzaglia A, Zamparini E, Leonetti P, Campos EC. Intravitreal vs. subtenon triamcinolone acetonide for the treatment of diabetic cystoid macular edema. BMC Ophthalmol. 2008. 8:5.
Article16. Ozdek S, Bahçeci UA, Gürelik G, Hasanreisoğlu B. Posterior subtenon and intravitreal triamcinolone acetonide for diabetic macular edema. J Diabetes Complications. 2006. 20:246–251.
Article17. Ferris FL 3rd, Kassoff A, Bresnick GH, Bailey I. New visual acuity charts for clinical research. Am J Ophthalmol. 1982. 94:91–96.
Article18. Chylack LT Jr, Wolfe JK, Singer DM, Leske MC, Bullimore MA, Bailey IL, et al. The Lens Opacities Classification System III. The Longitudinal Study of Cataract Study Group. Arch Ophthalmol. 1993. 111:831–836.19. Freeman WR, Green RL, Smith RE. Echographic localization of corticosteroids after periocular injection. Am J Ophthalmol. 1987. 103(3 Pt 1):281–288.
Article20. Ozkiris A, Evereklioglu C, Erkiliç K, Tamçelik N, Mirza E. Intravitreal triamcinolone acetonide injection as primary treatment for diabetic macular edema. Eur J Ophthalmol. 2004. 14:543–549.
Article21. Karacorlu M, Ozdemir H, Karacorlu S, Alacali N, Mudun B, Burumcek E. Intravitreal triamcinolone as a primary therapy in diabetic macular oedema. Eye. 2005. 19:382–386.
Article22. Moshfeghi DM, Kaiser PK, Scott IU, Sears JE, Benz M, Sinesterra JP, et al. Acute endophthalmitis following intravitreal triamcinolone acetonide injection. Am J Ophthalmol. 2003. 136:791–796.
Article23. Jonas JB, Kreissig I, Degenring R. Secondary chronic open-angle glaucoma after intravitreal triamcinolone acetonide. Arch Ophthalmol. 2003. 121:729–730.24. Roth DB, Chieh J, Spirn MJ, Green SN, Yarian DL, Chaudhry NA. Noninfectious endophthalmitis associated with intravitreal triamcinolone injection. Arch Ophthalmol. 2003. 121:1279–1282.
Article25. Rivellese M, George A, Sulkes D, Reichel E, Puliafito C. Optical coherence tomography after laser photocoagulation for clinically significant macular edema. Ophthalmic Surg Lasers. 2000. 31:192–197.
Article26. Kang SW, Park CY, Ham DI. The correlation between fluorescein angiographic and optical coherence tomographic features in clinically significant diabetic macular edema. Am J Ophthalmol. 2004. 137:313–322.
Article27. Browning DJ, McOwen MD, Bowen RM Jr, O'Marah TL. Comparison of the clinical diagnosis of diabetic macular edema with diagnosis by optical coherence tomography. Ophthalmology. 2004. 111:712–715.28. Brown JC, Solomon SD, Bressler SB, Schachat AP, DiBernardo C, Bressler NM. Detection of diabetic foveal edema: contact lens biomicroscopy compared with optical coherence tomography. Arch Ophthalmol. 2004. 122:330–335.29. Sadda SR, Tan O, Walsh AC, Schuman JS, Varma R, Huang D. Automated detection of clinically significant macular edema by grid scanning optical coherence tomography. Ophthalmology. 2006. 113:1187. e1-12.30. Chew E, Strauber S, Beck R, Aiello LP, Antoszyk A, Bressler N, et al. Randomized trial of peribulbar triamcinolone acetonide with and without focal photocoagulation for mild diabetic macular edema: a pilot study. Ophthalmology. 2007. 114:1190–1196.31. Brasil OF, Smith SD, Galor A, Lowder CY, Sears JE, Kaiser PK. Predictive factors for short-term visual outcome after intravitreal triamcinolone acetonide injection for diabetic macular oedema: an optical coherence tomography study. Br J Ophthalmol. 2007. 91:761–765.
Article32. Lee CM, Olk RJ. Modified grid laser photocoagulation for diffuse diabetic macular edema. Long-term visual results. Ophthalmology. 1991. 98:1594–1602.
Article33. Olk RJ. Modified grid argon (blue-green) laser photocoagulation for diffuse diabetic macular edema. Ophthalmology. 1986. 93:938–950.
Article34. Challa JK, Gillies MC, Penfold PL, Gyory JF, Hunyor AB, Billson FA. Exudative macular degeneration and intravitreal triamcinolone: 18 month follow up. Aust N Z J Ophthalmol. 1998. 26:277–281.
Article35. Chieh JJ, Roth DB, Liu M, Belmont J, Nelson M, Regillo C, et al. Intravitreal triamcinolone acetonide for diabetic macular edema. Retina. 2005. 25:828–834.
Article36. Avitabile T, Longo A, Reibaldi A. Intravitreal triamcinolone compared with macular laser grid photocoagulation for the treatment of cystoid macular edema. Am J Ophthalmol. 2005. 140:695–702.
Article37. Kang SW, Sa HS, Cho HY, Kim JI. Macular grid photocoagulation after intravitreal triamcinolone acetonide for diffuse diabetic macular edema. Arch Ophthalmol. 2006. 124:653–658.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intravitreal and Additional Posterior Subtenon Triamcinolone Injection in Diabetic Macular Edema
- The Effect of Intravitreal Triamcinolone Acetonide Injection according to the Diabetic Macular Edema Type
- Intravitreal versus Posterior Subtenon Injection of Triamcinolone Acetonide for Diabetic Macular Edema
- Surgical Removal of Sub-Tenon Triamcinolone Acetonide in Cases of Increased Intraocular Pressure after Sub-Tenon Injection
- Laser Photocoagulation Combined with Intravitreal Triamcinolone Acetonide Injection in Proliferative Diabetic Retinopathy with Macular Edema
