Multiple Myeloma with Biclonal Gammopathy Accompanied by Prostate Cancer
- Affiliations
-
- 1Department of Internal Medicine, Eulji University Hospital, Daejeon, Korea. lee982023@eulji.ac.kr
- 2Department of Laboratory Medicine, Eulji University Hospital, Daejeon, Korea.
- 3Department of Radiation Oncology, Eulji University Hospital, Daejeon, Korea.
- KMID: 1781694
- DOI: http://doi.org/10.3343/kjlm.2011.31.4.285
Abstract
- We report a rare case of multiple myeloma with biclonal gammopathy (IgG kappa and IgA lambda type) in a 58-year-old man with prostate cancer who presented with lower back pain. Through computed tomography (CT) imaging, an osteolytic lesion at the L3 vertebra and an enhancing lesion of the prostate gland with multiple lymphadenopathies were found. In the whole body positron emission tomography-computed tomography (PET-CT), an additional osteoblastic bone lesion was found in the left ischial bone. A prostate biopsy was performed, and adenocarcinoma was confirmed. Decompression surgery of the L3 vertebra was conducted, and the pathologic result indicated that the lesion was a plasma cell neoplasm. Immunofixation electrophoresis showed the presence of biclonal gammopathy (IgG kappa and IgA lambda). Bone marrow plasma cells (CD138 positive cells) comprised 7.2% of nucleated cells and showed kappa positivity. We started radiation therapy for the L3 vertebra lesion, with a total dose of 3,940 cGy, and androgen deprivation therapy as treatment for the prostate cancer.
MeSH Terms
-
Adenocarcinoma/complications/*diagnosis/radiotherapy
Antineoplastic Agents/therapeutic use
Bone Marrow Cells/metabolism/pathology
Combined Modality Therapy
Humans
Immunoelectrophoresis
Immunoglobulin kappa-Chains/blood
Immunoglobulin lambda-Chains/blood
Male
Middle Aged
Multiple Myeloma/complications/*diagnosis/drug therapy
Neoplasm Staging
Positron-Emission Tomography
Prostatic Neoplasms/complications/*diagnosis/radiotherapy
Spine/pathology
Syndecan-1/metabolism
Tomography, X-Ray Computed
Figure
-
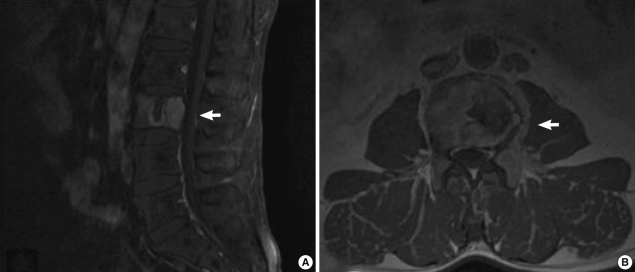
Fig. 1 Spinal magnetic resonance imaging (MRI). A plasma cell neoplasm compressing the spinal cord is seen in the L3 vertebral body. (A) Sagittal view. (B) Transverse view.
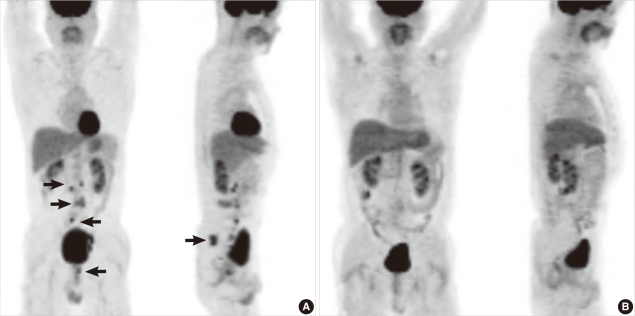
Fig. 2 PET-CT performed at diagnosis and follow-up at 27 months. (A) At diagnosis, increased FDP uptake was seen in the L3 vertebral body, the prostate gland, and ischial bone. Further, hypermetabolic activity was seen in the paraaortic, aortocaval, prevertebral, and left common iliac lymph nodes. These findings may suggest metastatic lymphadenopathies. Increased FDP uptake was seen in the ischial bone. (B) Follow-up PET-CT after 27 months. At the end of the follow-up, an improvement in intra-abdominal lymphadenopathies and disappearance of the hypermetabolic lesion in the prostate gland and ischial bone were observed.Abbreviations: PET-CT, positron emission tomography-computed tomography; FDP, fructose-1,6-bisphosphate.
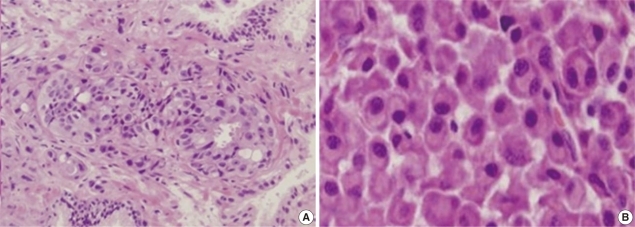
Fig. 3 (A) Prostate gland biopsy. It shows cancer infiltration of individual cells. It may suggest the presence of a gland-forming adenocarcinoma (Hematoxylin & Eosin, ×200). (B) L3 vertebral body biopsy. Some plasma cells show increased nuclear/cytoplasmic ratios, and they contain an eccentric nucleus and a peri-nuclear halo. Some other cells have double nuclei (Hematoxylin & Eosin, ×400).

Fig. 4 (A) Protein electrophoresis. An M-peak is seen in the gamma fraction. (B) Serum immunofixation electrophoresis. It shows biclonal gammopathy of IgG kappa type and IgA lambda type. (C) Urine immunofixation electrophoresis. It shows a dark band for kappa antisera.
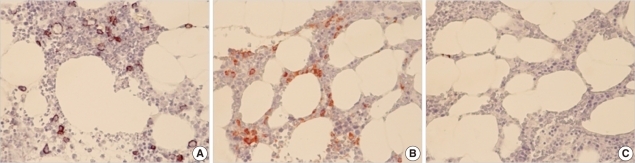
Fig. 5 Bone marrow immunohistochemical staining. (A) CD138 staining. About 7.2% of the marrow nucleated cells showed CD138 immunoreactivity. (B) Kappa staining. Positive staining of kappa light chains is shown. (C) Lambda staining. Negative staining of lambda light chains is shown.Abbreviation: CD, cluster of differentiation.
Reference
-
1. Rajkumar SV. Multiple myeloma: 2011 update on diagnosis, risk-stratification, and management. Am J Hematol. 2011; 86:57–65. PMID: 21181954.
Article2. Kyle RA, Robinson RA, Katzmann JA. The clinical aspects of biclonal gammopathies. Review of 57 cases. Am J Med. 1981; 71:999–1008. PMID: 6797297.3. Kao J, Jani AB, Vijayakumar S. Is there an association between multiple myeloma and prostate cancer? Med Hypotheses. 2004; 63:226–231. PMID: 15236779.
Article4. Huang E, Teh BS, Saleem A, Butler EB. Recurrence of prostate adenocarcinoma presenting with multiple myeloma simulating skeletal metastases of prostate adenocarcinoma. Urology. 2002; 60:1111. PMID: 12475684.
Article5. Terris MK, Hausdorff J, Freiha FS. Hematolymphoid malignancies diagnosed at the time of radical prostatectomy. J Urol. 1997; 158:1457–1459. PMID: 9302142.
Article6. Knobel D, Zouhair A, Tsang RW, Poortmans P, Belkacémi Y, Bolla M, et al. Prognostic factors in solitary plasmacytoma of the bone: a multicenter Rare Cancer Network study. BMC Cancer. 2006; 6:118. PMID: 16677383.
Article7. Mahto M, Balakrishnan P, Koner BC, Lali P, Mishra TK, Saxena A. Rare case of biclonal gammopathy. IJCRI. 2011; 2:11–14.
Article8. Kahr WH, Al-Homadhi A, Meharchand J, Bailey DJ, Stewart AK. Testicular plasmacytoma following chemical orchiectomy: potential role of hypogonadism in myeloma proliferation. Leuk Lymphoma. 1998; 28:437–442. PMID: 9517517.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Multiple Myeloma with Biclonal Gammopathy
- A Case of Multiple Myeloma with Biclonal Gammopathy
- A Case of Multiple Myeloma with Biclonal (IgG-K and IgA-K) M-proteins
- A Case of Lymphoplasmacytic Lymphoma/Waldenström's Macroglobulinemia with IgM-κ and IgA-λ Biclonal Gammopathy
- Clinical Application of (18)F-FDG PET in Multiple Myeloma
