Successful Treatment of Mycobacterium celatum Pulmonary Disease in an Immunocompetent Patient Using Antimicobacterial Chemotherapy and Combined Pulmonary Resection
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. wjkoh@skku.edu
- 2Department of Laboratory Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1779652
- DOI: http://doi.org/10.3349/ymj.2010.51.6.980
Abstract
- Mycobacterium celatum is a nontuberculous mycobacterium that rarely causes pulmonary disease in immunocompetent subjects. We describe the successful treatment of M. celatum lung disease with antimicobacterial chemotherapy and combined pulmonary resection. A 33-year-old woman was referred to our hospital with a 3-month history of a productive cough. Her medical history included pulmonary tuberculosis 14 years earlier. Her chest X-ray revealed a large cavitary lesion in the left upper lobe. The sputum smear was positive for acid-fast bacilli, and M. celatum was subsequently identified in more than three sputum cultures, using molecular methods. After 1 year of therapy with clarithromycin, ethambutol, and ciprofloxacin, the patient underwent a pulmonary resection for a persistent cavitary lesion. The patient was considered cured after receiving 12 months of postoperative antimycobacterial chemotherapy. There has been no recurrence of disease for 18 months after treatment completion. In summary, M. celatum is an infrequent cause of potentially treatable pulmonary disease in immunocompetent subjects. Patients with M. celatum pulmonary disease who can tolerate resectional surgery might be considered for surgery, especially in cases of persistent cavitary lesions despite antimycobacterial chemotherapy.
MeSH Terms
Figure
-
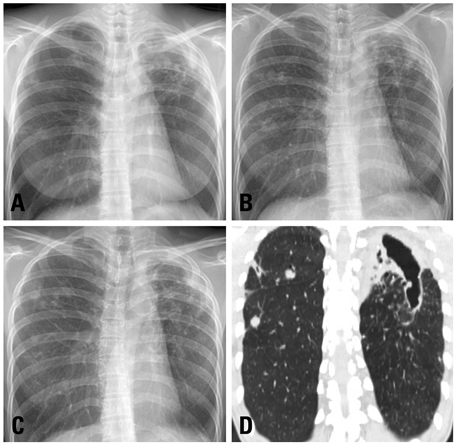
Fig. 1 A 35 year-old woman with Mycobacterium celatum lung disease. (A) The posteroanterior chest radiography at first visit shows a large cavitary lesion in the left upper lobe. Note the multiple nodular opacities involving the right lung. (B) The chest radiography at the subsequent revisit shows aggravation of the cavitation in the left upper lobe, as well as enlargement of the nodular lesions in the right lung. (C) The chest radiography taken after 12 months of antibiotic treatment shows that the size of the cavitary lesion in the left upper lobe is unchanged, although the multiple nodular lesions in the right lung have improved. (D) The chest computed tomography scan taken after 12 months of antibiotic treatment reveals a large remnant cavitary lesion that involves both the left upper lobe and the superior segment of the left lower lobe.
Reference
-
1. Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007. 175:367–416.
Article2. Koh WJ, Kwon OJ, Jeon K, Kim TS, Lee KS, Park YK, et al. Clinical significance of nontuberculous mycobacteria isolated from respiratory specimens in Korea. Chest. 2006. 129:341–348.
Article3. Park HY, Koh WJ, Kwon OJ, Lee NY, Shim YM, Park YK, et al. Pulmonary disease caused by Mycobacterium xenopi: the first case in Korea. Yonsei Med J. 2007. 48:871–875.
Article4. Park S, Suh GY, Chung MP, Kim H, Kwon OJ, Lee KS, et al. Clinical significance of Mycobacterium fortuitum isolated from respiratory specimens. Respir Med. 2008. 102:437–442.
Article5. Butler WR, O'Connor SP, Yakrus MA, Smithwick RW, Plikaytis BB, Moss CW, et al. Mycobacterium celatum sp. nov. Int J Syst Bacteriol. 1993. 43:539–548.6. Christiansen DC, Roberts GD, Patel R. Mycobacterium celatum, an emerging pathogen and cause of false positive amplified Mycobacterium tuberculosis direct test. Diagn Microbiol Infect Dis. 2004. 49:19–24.
Article7. Bux-Gewehr I, Hagen HP, Rüsch-Gerdes S, Feurle GE. Fatal pulmonary infection with Mycobacterium celatum in an apparently immunocompetent patient. J Clin Microbiol. 1998. 36:587–588.
Article8. Tjhie JH, van Belle AF, Dessens-Kroon M, van Soolingen D. Misidentification and diagnostic delay caused by a false-positive amplified Mycobacterium tuberculosis direct test in an immunocompetent patient with a Mycobacterium celatum infection. J Clin Microbiol. 2001. 39:2311–2312.
Article9. Piersimoni C, Zitti PG, Nista D, Bornigia S. Mycobacterium celatum pulmonary infection in the immunocompetent: case report and review. Emerg Infect Dis. 2003. 9:399–402.
Article10. Kim DK, Kim BJ, Kook YH, Lee CT, Yoo CG, Kim YW, et al. Pulmonary infection with Mycobacterium celatum in immunocompetent host: The first case report in Korea. Tuberc Respir Dis. 1999. 47:697–703.
Article11. Lee H, Park HJ, Cho SN, Bai GH, Kim SJ. Species identification of mycobacteria by PCR-restriction fragment length polymorphism of the rpoB gene. J Clin Microbiol. 2000. 38:2966–2971.
Article12. National Committee for Clinical Laboratory Standards. Document No. M24-A. Susceptibility testing of mycobacteria, nocardiae, and other aerobic actinomycetes; Approved Standard. 2003. Wayne, PA: NCCLS.13. Bull TJ, Shanson DC, Archard LC, Yates MD, Hamid ME, Minnikin DE. A new group (type 3) of Mycobacterium celatum isolated from AIDS patients in the London area. Int J Syst Bacteriol. 1995. 45:861–862.14. Emler S, Praplan P, Rohner P, Auckenthaler R, Hirschel B. Disseminated infection with Mycobacterium celatum. Schweiz Med Wochenschr. 1996. 126:1062–1065.15. Zurawski CA, Cage GD, Rimland D, Blumberg HM. Pneumonia and bacteremia due to Mycobacterium celatum masquerading as Mycobacterium xenopi in patients with AIDS: an underdiagnosed problem? Clin Infect Dis. 1997. 24:140–143.16. Fattorini L, Baldassarri L, Li YJ, Ammendolia MG, Fan Y, Recchia S, et al. Virulence and drug susceptibility of Mycobacterium celatum. Microbiology. 2000. 146:2733–2742.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary infection with Mycobacterium celatum in immunocompetent host: The first case report in Korea
- A Case of Pulmonary and Endobronchial Mycobacterium avium Infection Presenting as an Acute Pneumonia in an Immunocompetent Patient
- Successful Pulmonary Resection Combined with Chemotherapy for the Treatment of Mycobacterium avium Pulmonary Disease: A Case Report
- Mycobacterium avium Infection Presenting as Endobronchial Lesions in an Immunocompetent Patient
- Pulmonary Malakoplakia Associated with Peripheral Cysts in an Immunocompetent Patient: A Case Report
