Ultrasonographic Measurement of the Ligamentum Flavum Depth; Is It a Reliable Method to Distinguish True and False Loss of Resistance?
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Chungnam National University Hospital, Daejeon, Korea. whlee@cnu.ac.kr
- KMID: 1778993
- DOI: http://doi.org/10.3344/kjp.2012.25.2.99
Abstract
- BACKGROUND
Previous studies have shown that if performed without radiographic guidance, the loss of resistance (LOR) technique can result in inaccurate needle placement in up to 30% of lumbar epidural blocks. To date, no study has shown the efficacy of measuring the depth of the posterior complex (ligamentum flavum, epidural space, and posterior dura) ultrasonographically to distinguish true and false LOR.
METHODS
40 cervical epidural blocks were performed using the LOR technique and confirmed by epidurograms. Transverse ultrasound images of the C6/7 area were taken before each cervical epidural block, and the distances from the skin to the posterior complex, transverse process, and supraspinous ligament were measured on each ultrasound view. The number of LOR attempts was counted, and the depth of each LOR was measured with a standard ruler. Correlation of false and true positive LOR depth with ultrasonographically measured depth was also statistically analyzed.
RESULTS
76.5% of all cases (26 out of 34) showed false positive LOR. Concordance correlation coefficients between the measured distances on ultrasound (skin to ligamentum flavum) and actual needle depth were 0.8285 on true LOR. Depth of the true positive LOR correlated with height and weight, with a mean of 5.64 +/- 1.06 cm, while the mean depth of the false positive LOR was 4.08 +/- 1.00 cm.
CONCLUSIONS
Ultrasonographic measurement of the ligamentum flavum depth (or posterior complex) preceding cervical epidural block is beneficial in excluding false LOR and increasing success rates of cervical epidural blocks.
Keyword
Figure
-

Fig. 1 Transverse ultrasonographic image at the level of C6-7. Each number indicates supraspinous ligament (1), transverse process (2), ligament flavum (3), posterior dura (4), anterior complex (anterior dura, posterior longitudinal ligament, vertebral body)(5).

Fig. 2 Lateral fluroscopic images of cervical epidural block at the level of C6-7. Note that the contrast medium spread show non-epidural pattern (A) and epidural pattern (B) on a same patient.
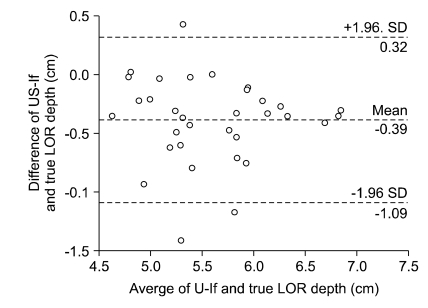
Fig. 3 Bland-Altman precision analysis of the measured differences between ultrasound-measured depth of skin to ligamentum flavum and depth of true loss of. LOR: loss of resistance, US-lf: measured depth from skin to ligamentum flavum or posterior complex.

Fig. 4 Concordance correlation between ultrasound-measured depth of skin to ligament flavum and depth of compensated true loss of resistance. LOR: loss of resistance, US-lf: measured depth from skin to ligament flavum or posterior complex.
Cited by 2 articles
-
Vertebral level of Tuffier's line measured by ultrasonography in parturients in the lateral decubitus position
Se Hee Kim, Dong Yeon Kim, Jong In Han, Hee Jung Baik, Hahck Soo Park, Guie Yong Lee, Jong Hak Kim
Korean J Anesthesiol. 2014;67(3):181-185. doi: 10.4097/kjae.2014.67.3.181.Ultrasound Sonography at the Pain Clinic in Korea: Past, Present and Future
Ji Yong Park
Korean J Pain. 2013;26(1):1-2. doi: 10.3344/kjp.2013.26.1.1.
Reference
-
1. Castagnera L, Maurette P, Pointillart V, Vital JM, Erny P, Sénégas J. Long-term results of cervical epidural steroid injection with and without morphine in chronic cervical radicular pain. Pain. 1994; 58:239–243. PMID: 7816491.
Article2. Ferrante FM, Wilson SP, Iacobo C, Orav EJ, Rocco AG, Lipson S. Clinical classification as a predictor of therapeutic outcome after cervical epidural steroid injection. Spine (Phila Pa 1976). 1993; 18:730–736. PMID: 8516703.
Article3. Rowlingson JC, Kirschenbaum LP. Epidural analgesic techniques in the management of cervical pain. Anesth Analg. 1986; 65:938–942. PMID: 3017152.
Article4. Waldman SD. Cervical epidural abscess after cervical epidural nerve block with steroids. Anesth Analg. 1991; 72:717–718. PMID: 2018238.
Article5. Williams KN, Jackowski A, Evans PJ. Epidural haematoma requiring surgical decompression following repeated cervical epidural steroid injections for chronic pain. Pain. 1990; 42:197–199. PMID: 1701045.
Article6. Abram SE, O'Connor TC. Complications associated with epidural steroid injections. Reg Anesth. 1996; 21:149–162. PMID: 8829408.7. Hodges SD, Castleberg RL, Miller T, Ward R, Thornburg C. Cervical epidural steroid injection with intrinsic spinal cord damage. Two case reports. Spine (Phila Pa 1976). 1998; 23:2137–2142. PMID: 9794061.8. White AH. Injection techniques for the diagnosis and treatment of low back pain. Orthop Clin North Am. 1983; 14:553–567. PMID: 6223258.
Article9. Hogan QH. Epidural anatomy examined by cryomicrotome section. Influence of age, vertebral level, and disease. Reg Anesth. 1996; 21:395–406. PMID: 8895998.10. Stojanovic MP, Vu TN, Caneris O, Slezak J, Cohen SP, Sang CN. The role of fluoroscopy in cervical epidural steroid injections: an analysis of contrast dispersal patterns. Spine (Phila Pa 1976). 2002; 27:509–514. PMID: 11880836.11. Kim SH, Lee KH, Yoon KB, Park WY, Yoon DM. Sonographic estimation of needle depth for cervical epidural blocks. Anesth Analg. 2008; 106:1542–1547. PMID: 18420873.
Article12. Fredman B, Nun MB, Zohar E, Iraqi G, Shapiro M, Gepstein R, et al. Epidural steroids for treating "failed back surgery syndrome": is fluoroscopy really necessary? Anesth Analg. 1999; 88:367–372. PMID: 9972758.13. Wulf H, Kibbel K, Mercker S, Maier C, Gleim M, Crayen E. Radiologic position control of epidural catheters (epidurography). An instrument of quality assurance for regional analgesia. Anaesthesist. 1993; 42:536–544. PMID: 8368475.14. Cork RC, Kryc JJ, Vaughan RW. Ultrasonic localization of the lumbar epidural space. Anesthesiology. 1980; 52:513–516. PMID: 7377598.
Article15. Wallace DH, Currie JM, Gilstrap LC, Santos R. Indirect sonographic guidance for epidural anesthesia in obese pregnant patients. Reg Anesth. 1992; 17:233–236. PMID: 1515392.16. Arzola C, Davies S, Rofaeel A, Carvalho JC. Ultrasound using the transverse approach to the lumbar spine provides reliable landmarks for labor epidurals. Anesth Analg. 2007; 104:1188–1192. PMID: 17456672.
Article17. Balki M, Lee Y, Halpern S, Carvalho JC. Ultrasound imaging of the lumbar spine in the transverse plane: the correlation between estimated and actual depth to the epidural space in obese parturients. Anesth Analg. 2009; 108:1876–1881. PMID: 19448216.
Article18. Bonazzi M, Bianchi De Grazia L, Di Gennaro S, Lensi C, Migliavacca S, Marsicano M, et al. Ultrasonography-guided identification of the lumbar epidural space. Minerva Anestesiol. 1995; 61:201–205. PMID: 7478051.19. Ferre RM, Sweeney TW, Strout TD. Ultrasound identification of landmarks preceding lumbar puncture: a pilot study. Emerg Med J. 2009; 26:276–277. PMID: 19307389.
Article20. Chin KJ, Perlas A, Singh M, Arzola C, Prasad A, Chan V, et al. An ultrasound-assisted approach facilitates spinal anesthesia for total joint arthroplasty. Can J Anaesth. 2009; 56:643–650. PMID: 19548051.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anatomic Variations of Cervical and High Thoracic Ligamentum Flavum
- Comparison of Methods to Confirm the Cervical Epidural Space
- Focal Ligamentum Flavum Hypertrophy with Ochronotic Deposits: An Unusual Cause for Neurogenic Claudication in Alkaptonuria
- As a Cause of Myelopathy in the Lower Thracic Spines ): Two Cases Report
- Thoracic Myelopathy Due to Ossification of Ligamentum Flavum: Three cases Report
