J Korean Med Sci.
2006 Jun;21(3):567-571. 10.3346/jkms.2006.21.3.567.
A Successful Live Birth Through in vitro Fertilization Program After Conservative Treatment of FIGO Grade I Endometrial Cancer
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Keimyung University, School of Medicine, Daegu, Korea. rl670416@dsmc.or.kr
- KMID: 1778447
- DOI: http://doi.org/10.3346/jkms.2006.21.3.567
Abstract
- Infertile women with chronic anovulation are prone to be exposed to unopposed estrogen stimulation and have the high risk of being suffering from endometrial hyperplasia or even endometrial carcinoma. A few reports have suggested that nulliparous young women (under 40 yr of age) with endometrial carcinoma could be treated conservatively to preserve fertility and succeed the live birth. We report on a 36-yr-old woman who received conservative treatment of endometrial carcinoma (stage I, grade 1) by curettage and progestin. After megestrol medication of total 71,680 mg during 24 weeks, we found the regression of endometrial lesion by curettage and hysteroscopic examination. Then we decided to perform in vitro fertilization program. Two embryos were transferred and heterotypic pregnancy was diagnosed 27 days after embryo transfer. After right salpingectomy, she received routine obstetrical care and delivered by cesarean section at 38 weeks in gestational periods. Two years after delivery, she is healthy without any evidence of recurrent disease. The fertility preserving treatment is an option in endometrial cancer patients if carefully selected, and assisted reproductive technologies would be helpful.
MeSH Terms
Figure
-
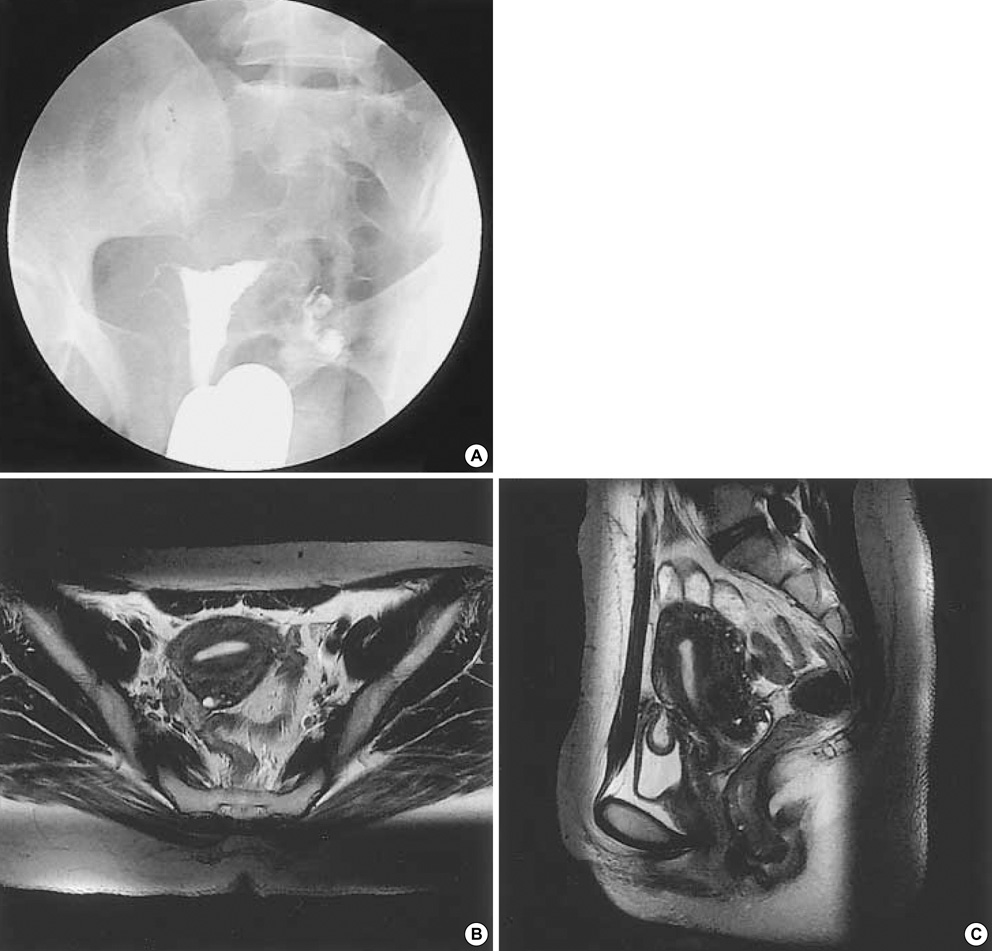
Fig. 1 (A) Hysterosalpingogram shows a small filling defect in the uterine cavity. (B and C) MRI reveals no residual tumor in the endometrium nor myometrial involvement after curettage.
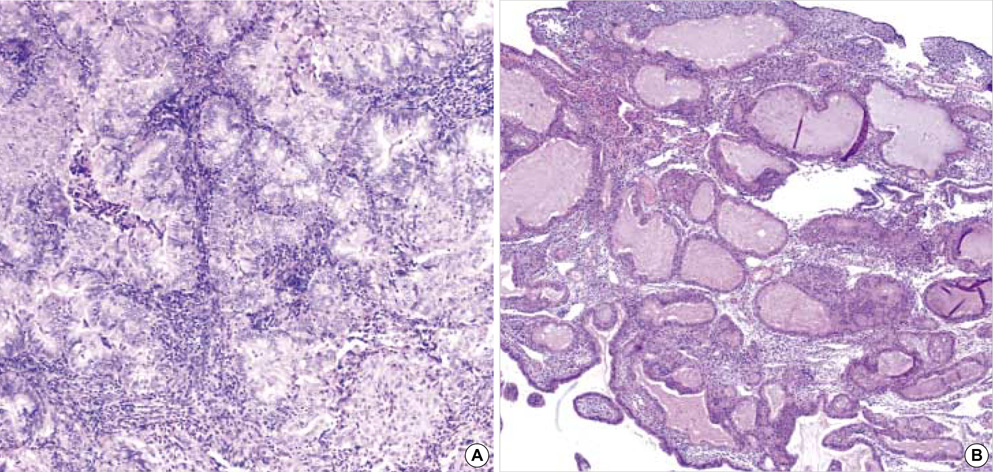
Fig. 2 (A) A well-differentiated endometrioid adenocarcinoma. Light micrograph shows anaplastic proliferation of the endometrial glands associated with foci of squamoid differentiation (H&E stain, ×200). (B) After progestin therapy for 8 weeks, the endometrium shows complex hyperplasia without nuclear atypia in the dilated endometrial glands (H&E stain, ×200).
Reference
-
1. Ostor AG, Adam R, Gutteridge BH, Fortune DW. Endometrial carcinoma in young women. Aust N Z J Obstet Gynecol. 1982. 22:38–42.
Article2. Hull MG, Glazener CM, Kelly NJ, Conway DI, Foster PA, Hinton RA, Coulson C, Lambert PA, Watt EM, Desai KM. Population study of causes, treatment, and outcome of infertility. Br Med J. 1985. 291:1693–1697.
Article3. Ron E, Lunenfeld B, Menczer J, Blumstein T, Katz L, Oelsner G, Serr D. Cancer incidence in a cohort of infertile women. Am J Epidemiol. 1987. 125:780–790.
Article4. Meirow D, Schenker JG. The link between female infertility and cancer: epidemiology and possible aetiologies. Hum Reprod Update. 1996. 2:63–75.
Article5. Salha O, Martin-Hirsch P, Lane G, Sharma V. Endometrial carcinoma in a young patient with polycystic ovarian syndrome: first suspected at time of embryo transfer. Hum Reprod. 1997. 12:959–962.
Article6. Emons G, Heyl W. Hormonal treatment of endometrial cancer. J Cancer Res Clin Oncol. 2000. 126:619–623.
Article7. Lowe MP, Bender D, Sood AK, Davis W, Syrop CH, Sorosky JI. Two successful pregnancies after conservative treatment of endometrial cancer and assisted reproduction. Fertil Steril. 2002. 77:188–189.
Article8. Farhi DC, Nosanchuk J, Silverberg SG. Endometrial adenocarcinoma in women under 25 years of age. Obstet Gynecol. 1986. 68:741–745.
Article9. Randall TC, Kurman RJ. Progestin treatment of atypical hyperplasia and well differentiated carcinoma of the endometrium in women under age 40. Obstet Gynecol. 1997. 90:434–440.10. Kim YB, Holschneider CH, Ghosh K, Nieberg RK, Montz FJ. Progestin alone as primary treatment of endometrial carcinoma in premenopausal women. Cancer. 1997. 79:320–327.
Article11. Kimmig R, Strowitzki T, Muller-Hocker J, Kurzl R, Korell M, Hepp H. Conservative treatment of endometrial cancer permitting subsequent triplet pregnancy. Gynecol Oncol. 1995. 58:255–257.
Article12. Mitsushita J, Toki T, Kato K, Fujii S, Konishi I. Endometrial carcinoma remaining after term pregnancy following conservative treatment with medroxyprogesterone acetate. Gynecol Oncol. 2000. 79:129–132.
Article13. Jobo T, Imai M, Kawaguchi M, Kenmochi M, Kuramoto H. Successful conservative treatment of endometrial carcinoma permitting subsequent pregnancy: report of two cases. Eur J Gynaecol Oncol. 2000. 21:119–122.14. Greenblatt RB, Gambrell RD Jr, Stoddard LD. The protective role of progesterone in the prevention of endometrial cancer. Pathol Res Pract. 1982. 174:297–318.
Article15. Daniel AG, Peters WA. Accuracy of office and operating room curettage in the grading of endometrial carcinoma. Obstet Gynecol. 1988. 71:612–614.16. Larson DM, Johnson KK, Broste SK, Krawisz BR, Kresl JJ. Comparison of D&C and office endometrial biopsy in predicting final histopathologic grade in endometrial cancer. Obstet Gynecol. 1995. 86:38–42.17. Pinto AB, Gopal M, Herzog TJ, Pfeifer JD, Williams DB. Successful in vitro fertilization pregnancy after conservative management of endometrial cancer. Fertil Steril. 2001. 76:826–829.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Live birth in a woman with recurrent implantation failure and adenomyosis following transfer of refrozen-warmed embryos
- The Efficacy of Intracytoplasmic Sperm Injection for Previous Fertilization Failure with Conventional In Vitro Fertilization
- Histopathological profile of women who had previously failed in-vitro fertilization and the association to the outcome in the subsequent in-vitro fertilization cycle
- Endometrial adenocarcinoma in a 13-year-old girl
- The value of ultrasonographic endometrial measurement inthe prediction of pregnancy outcome in in vitro fertilization
